EHR Data Migration: Challenges, Risks, and Best Practices
EHR data migration is more than moving patient records from one system to another. It requires preserving data accuracy, maintaining clinical workflows, ensuring regulatory compliance, and minimizing downtime. Poor planning, incomplete data mapping, and inadequate testing are among the leading causes of migration failures. This guide explains the common risks of EHR data migration and outlines proven strategies and best practices to ensure a secure, successful, and disruption-free transition.
Why Healthcare Organizations Migrate EHR Systems?
No health system opts for EHR Data Migration because it wants to. The pressure comes from outside.
- Mergers and acquisitions:
Consolidated systems cannot run coordinated care on fragmented record environments. Post-merger, unified patient data is not a preference. It is a legal and clinical requirement. - Legacy modernization:
Old platforms fail ONC Cures Act mandates. They block HL7 FHIR API access. They cannot handle the data volumes modern health networks generate. Replacement becomes mandatory, not optional. - Vendor replacement:
Sometimes when a vendor gets acquired, discontinues a product line, or prices an organization out entirely, decisions pile up fast. The choices shrink. An organization that could wait months for a solution last year now has quarters, or weeks - Regulatory requirements:
Federal compliance programs and strict information-blocking mandates dictate specific EHR data capabilities. Legacy platforms simply lack the baseline architecture required to support these modern specifications.
The driver changes. The complexity of the migration does not. And none of these pressures make migration simpler.
What Data Needs Migration?
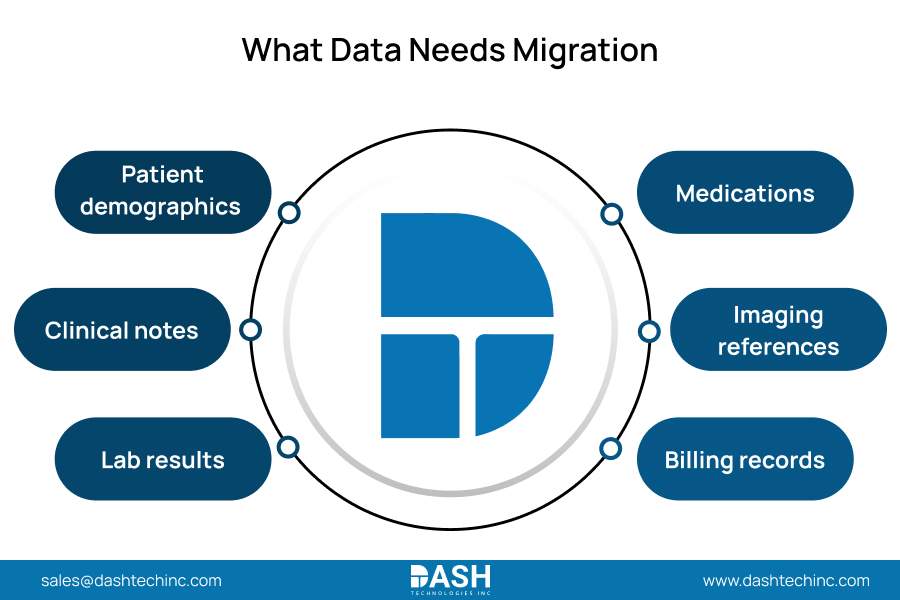
The scope here is bigger than most planning committees expect at kickoff. Clinical data does not exist in neat, portable buckets. It sits in relational structures that break when fields do not map correctly.
- Patient demographics:
The identity layer. Name, DOB, insurance, contact records. Every downstream clinical record depends on this foundation being accurate. - Clinical notes:
Physician documentation, discharge summaries, progress notes. The longitudinal patient story. Lose fidelity here, and clinicians make decisions on incomplete histories. - Lab results:
Historical and active data, with reference ranges and result flags that must survive the transfer intact. A stripped flag is a missed alert. - Medications:
Prescriptions, allergy records, dosing history. This is where mapping errors stop being technical problems and start being patient safety events. - Imaging references:
DICOM links, radiology reports, study metadata. These must trace back to the source archive. Gaps here are invisible until a clinician needs a prior scan. - Billing records:
Encounter data, claim histories, procedure codes. Revenue cycle continuity and audit readiness both depend on this data surviving in full.
Organizations that underestimate this scope at planning discover the gap at go-live, when fixing it is maximally disruptive.
Migrate Your EHR with Confidence
Ensure a secure, compliant, and disruption-free EHR data migration with expert planning, validation, and interoperability support.
Talk to Our ExpertsCommon Migration Risks
Published research on EHR-to-EHR transitions is unambiguous: migration challenges are not edge cases. They are predictable. They show up in the same places, in the same order, for almost every organization that runs this process without a disciplined framework.
- Data loss: Incomplete field mapping leaves records in the legacy system. Clinicians post-cutover work without critical patient histories. This is not a technical inconvenience. It is a care quality failure.
- Downtime: When scheduling, clinical workflows, and revenue cycle all go offline at once, there is no clean boundary around the disruption. It spreads.
- Mapping errors: The structural differences between source and target EHRs corrupt records at scale. Medication dosages misread, lab flags stripped, allergy codes gone. These errors do not announce themselves.
- Compliance violations: PHI outside HIPAA-compliant transfer pipelines creates direct regulatory exposure under 45 CFR 164. Add the ONC information-blocking provisions, and migration teams are managing two compliance dimensions most underweight.
- User adoption failures: Clinicians who get no workflow preparation default to workarounds. Those workarounds degrade data quality for years post-launch, long after the migration “succeeded.”
None of this surfaces at go-live. It accumulates silently in planning, then detonates when the organization is least equipped to absorb it.
Step-by-Step Migration Framework
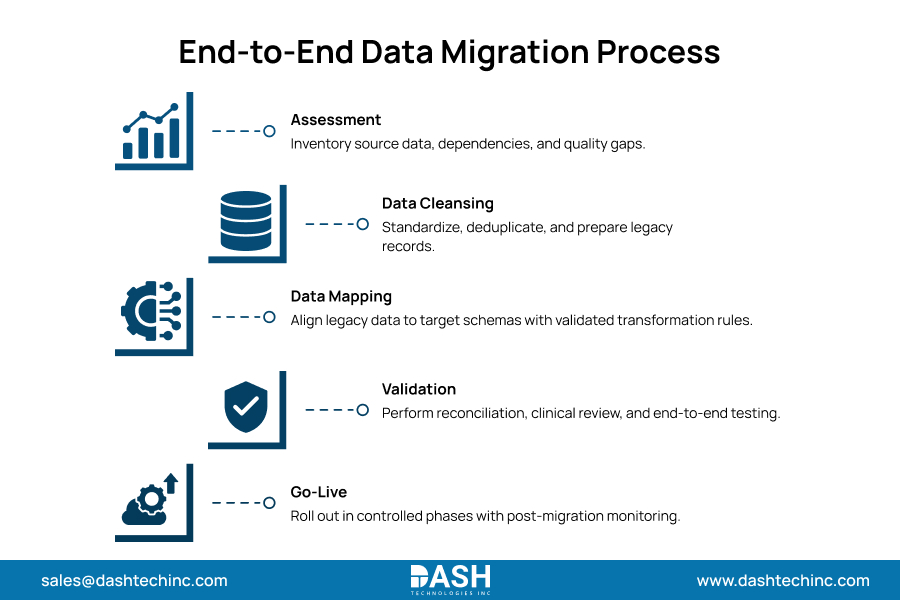
Structured execution removes improvisation from a process that cannot afford it.
- Assessment
Start here, and take your time. Before a single record moves, inventory every data asset in the source system: types, volumes, formats, dependencies. Then profile the data quality. Most organizations skip profiling and pay for it. What looks like a clean source system almost always has gaps, duplicates, and fields with no clear owner. - Cleansing
Legacy data is messier than anyone expects. Duplicate records, conflicting entries, data nobody has touched in a decade. All of it needs a decision before migration begins. The rule: dirty data moved into a clean system stays dirty. You do not solve data quality problems by changing platforms. - Mapping
This is where migrations actually fail. Every field in the legacy system needs an explicit decision: migrate it, transform it, archive it, or leave it behind. Whatever has no documented mapping becomes a failure at go-live. Technical architects and clinical subject matter experts both need seats at this table. One group without the other produces incomplete, often dangerous output. - Validation
Real data, not samples. Run the full parallel test environment with actual patient records and have clinical stakeholders sign off before any go-live authorization. Automated checks find structural mismatches. They will not find the semantic errors, the ones where a field moved correctly but now means something different in the target system. That takes a clinician. - Go-Live
Migrating department by department, or service line by service line, keeps the failure surface contained. Healthcare provider organizations that execute a full hard cutover and hit an issue in production have no clean path back. The blast radius is the entire organization.
Migration Best Practices
- Start with Governance
The steering committee exists before any technical work starts. Clinical leadership, IT, compliance, legal: all in the room, with actual decision authority. Every call that follows, from data retention policy to rollback thresholds, needs cross-functional ownership to stick. Organizations that skip this structure discover it mid-migration, when nobody can agree on who gets to make the call. - Maintain Audit Trails
Log every transformation applied to data during migration. Not because it feels thorough. Because HIPAA requires it, and ONC enforcement shows regulators scrutinize the process, not just the end state. If PHI moved through a pipeline and there is no documented trail, the organization cannot prove it was handled correctly. - Automate Validation
You cannot manually verify 10 million records without introducing the errors you are supposed to catch. Automated pipelines run rule-based checks across the full dataset in real time, flag anomalies, and produce documentation compliance reviews that actually need. Build this into the architecture before migration starts. Retrofitting it adds cost and delays go-live. - Use Experienced Integration Teams
Research on the science of EHR transitions makes it clear: the difficulty of migration is universal among clinicians, operations teams, and IT. What determines outcomes is the engineering depth behind the process. HL7 FHIR, API architecture, and the specific data models of both source and target systems. This expertise takes years to build. A live migration is not the place to develop it. - Prioritize Critical Data
Sequence matters a lot. Medications, allergies, active problem lists, and pending orders migrate first, with the tightest validation cycles. Historical administrative records and archived billing data go last. Organizing migration by clinical criticality keeps the highest-stakes records error-free and gives teams the right focus at each phase.
Common Mistakes to Avoid
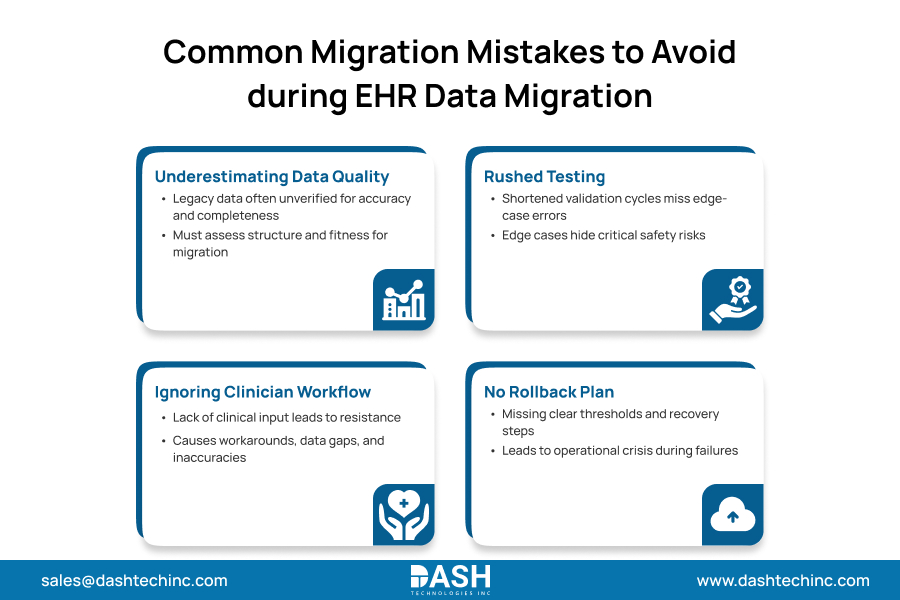
Most migration failures trace back to decisions made early, not problems that emerged late.
The biggest one: underestimating data quality. Legacy systems hold data nobody has audited in years. Assessment needs to include structural profiling, not just cataloguing what exists, but determining whether it is accurate, complete, and fit to migrate.
Testing gets compressed next. Schedule pressure pushes organizations to abbreviate validation cycles. That compression moves errors into production. Testing has to run long enough to catch edge-case mapping failures, not just confirm that standard records transfer. The edge cases are where the patient safety events hide.
Clinician workflow gets ignored last, and it costs the most over time. New documentation structures imposed without clinical input generate resistance. The resistance shows up as workarounds. The workarounds show up in the data as gaps and inaccuracies that compound for years.
And then there are the organizations that go live with no rollback plan. No defined thresholds, no tested recovery procedure, no named owners. When something fails in production (and something always does), they have no structured exit. A manageable migration problem becomes an operational crisis with no path out.
Conclusion
EHR data migration is a dividing line. Health systems that cross it successfully treat the process as a clinical and operational priority, full stop. Not an IT project with a delivery date. Governance, phased execution, and engineering depth are the infrastructure that makes that possible.
Our teams bring the interoperability expertise, clinical systems knowledge, and integration infrastructure health systems need to run EHR migrations without compromising data integrity or operational continuity. Contact us today!
About Dash
Dash Technologies Inc.
We’re technology experts with a passion for bringing concepts to life. By leveraging a unique, consultative process and an agile development approach, we translate business challenges into technology solutions Get in touch.






