
EHR Integration Cost Explained: What Hospitals Should Budget For in 2026
EHR integration cost looks like a single line on the budget. It isn’t. Underneath that one number sit a dozen choices nobody flagged in the kickoff meeting. So, a hospital signs for one figure and watches a bigger one show up by go-live. And the vendor usually didn’t cause it.
The blame lands on the lab system nobody listed, the workflow nobody mapped, the HIPAA work somebody assumed was “included.” Here’s the upside: none of that has to be a surprise. Break the spend into its real parts, and your 2026 number stops drifting.
What Hospitals Actually Budget?
What you pay tracks the size and mess of your environment. A solo cardiology practice bolting on a billing feed sits nowhere near a five-hospital system stitching together clinical data. Use these as planning anchors. They are not quotes.
| Hospital Size | Typical Budget |
| Small Practice | $10K–$50K |
| Community Hospital | $50K–$250K |
| Health System | $250K–$1M+ |
Custom work moves these fast. Read the low end as a tidy, API-friendly hookup. Read the high-end as deep workflow integration wired across a lot of endpoints.
Why EHR Integration Costs Vary So Much?
Two hospitals of the same size can finish $400K apart. Four things explain most of that gap.
- Number of systems: Every lab, pharmacy, imaging, and billing platform you bolt on is another interface. Each one gets built, then tested, then maintained.
- Vendor APIs: Modern FHIR endpoints save you. Old HL7 feeds and proprietary formats don’t, and the custom translation they demand burns hours fast.
- Custom workflows: Out-of-the-box rarely matches how your people actually order labs or route a note. Want a closer fit? That’s more engineering.
- Compliance requirements: HIPAA, your state’s privacy rules, and audit logging. Buyers forget this scope constantly, then find it on the invoice.
Pin those four down before you sign. They explain nearly every overrun we’ve seen.
Major Cost Components
A real estimate splits the job into stages. Leave one off the page, and you still pay for it later. You just pay more.
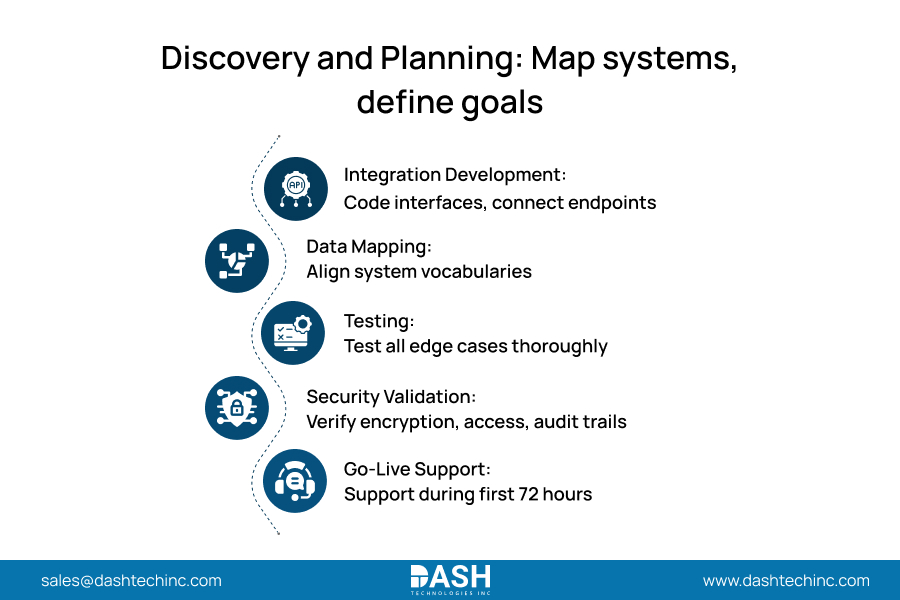
- Discovery and Planning
Engineers map your systems, trace the data flows, and agree on what “done” means. Shortchange this, and every stage after it inherits the mess. - Integration Development
The build itself. Interfaces get coded, endpoints get wired, and the bill scales straight off the system count you set during discovery. - Data Mapping
Your lab names a field one thing. The EHR names it another. Lining that vocabulary across every system is slow, fussy work, and it determines whether clinicians believe what’s on the screen. - Testing
Throw real edge cases at every interface before a patient chart depends on it. Skimp here to save a little now, and you’ll buy a production failure later. - Security Validation
Encryption, access controls, and audit trails, all checked against HIPAA. Regulators don’t grade this on a curve, and neither should you. - Go-Live Support
Engineers stand by at cutover for whatever testing is missed. Those first 72 hours decide one thing: whether staff trust the system or quietly work around it.
Cost by Integration Method
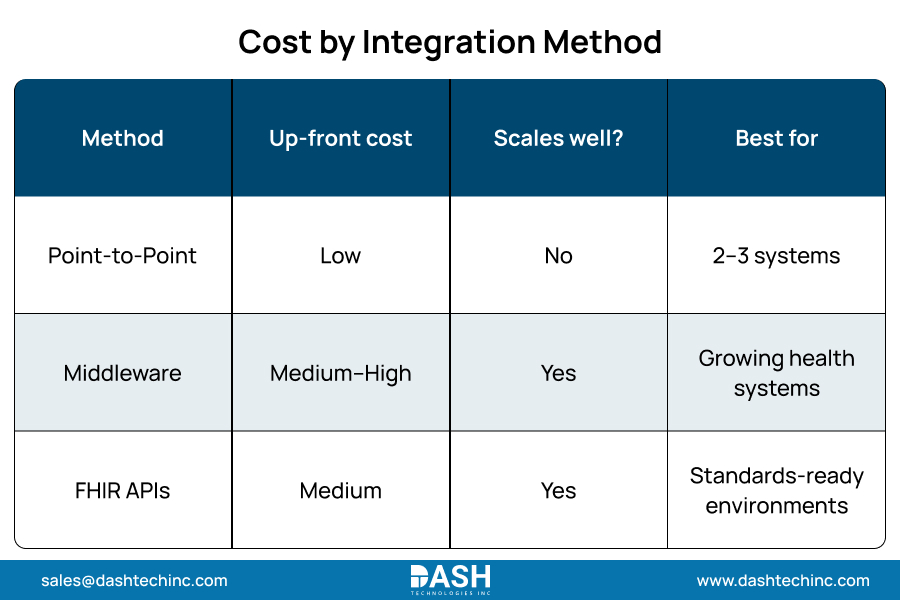
How you connect matters as much as what you connect. Three approaches run the field, and each one hands you a different cost curve.
- Point-to-point wires each system straight to the next. Cheap and quick for two or three links. Now add a tenth system. The tangle of connections turns into a maintenance trap, because one change ripples through all of them.
- Middleware sends everything through a central engine. Costs more on day one. Pays it back as you grow, since the next system plugs into the hub instead of into everything else.
- FHIR APIs lean on the HL7 standard built for exchanging health data. Best long-term economics of the three. And adoption already shows it: by 2022, roughly 70% of hospitals were using a FHIR API so patients could reach their own records, per ONC. Where your systems speak FHIR, start there.
Hidden Costs Hospitals Often Miss
The contract pays for the build. These show up after the ink dries, and they’re what blow up budgets that stopped counting at development.
- User training: Clinicians must learn the new workflow, and that learning curve costs you in coverage and lost productivity.
- Change management: No owner for rollout and communication? Adoption stalls, and the pushback wins.
- Vendor fees: Some platforms meter you per transaction or per connection. The meter never sleeps.
- API licensing: A few endpoints carry recurring access fees that stack up across systems.
- Ongoing maintenance: Interfaces break whenever either side ships an update. Budget for the engineers who keep them breathing.
Plan for all five on day one. None of them are surprises. They’re just the part that the vendor left off the slide one.
The ROI of EHR Integration
Integration isn’t a cost center. It’s a productivity engine, and the payback lands in numbers your CFO already watches.
Take the clinician for the first time. Physicians burn close to six hours of an eleven-hour day inside the EHR, and clerical and admin tasks eat 44% of that time. Connect the systems, and you kill the double entry, handing those hours back to actual patient care.
Now revenue. The American Hospital Association reports that denied claims cost health systems nearly $20 billion annually strictly in manual appeal overhead. Architecting clean, automated data exchanges between clinical and billing infrastructure directly eliminates the systemic coding errors generating these initial denials.
Faster throughput and sharper clinician focus follow the same thread. Every handoff you automate is a delay you just deleted. For healthcare providers living on thin margins, that’s the whole argument.
Build Your Own Cost Estimate
Before you dial a vendor, answer four questions. The answers turn a vague worry into a budget you can defend.
- Systems involved: List every platform that has to trade data. Yes, including the one IT always forgets.
- Number of interfaces: Count connections, not systems. One system needs three.
- Data migration required: Are you moving years of historical records, or only wiring up live feeds? Migration adds real scope.
- Compliance requirements: Write down the HIPAA and state obligations that hit your data in your region.
Show up with those four answers and you run the conversation. Show up without them and the estimate runs you. Integration partners strictly price against defined architectures; precise technical inputs directly generate accurate financial models.
Conclusion
EHR integration costs become entirely predictable once segmented by specific deployment phases and technical methods, fully accounting for the hidden maintenance dependencies that consistently derail unprepared launches. Scope all three and protect your margins and your timeline. Guess at them and you pay twice. So, map your systems, price each method against the way you actually plan to grow, and budget for the work that outlives go-live.
Need an accurate integration budget? Get a detailed integration assessment built around your technology stack.
Frequently Asked Questions
About Dash
Dash Technologies Inc.
We’re technology experts with a passion for bringing concepts to life. By leveraging a unique, consultative process and an agile development approach, we translate business challenges into technology solutions Get in touch.






