FHIR API Development Guide for Healthcare Applications
FHIR API development is federal law, not a modernization trend. As of January 1, 2023, the 21st Century Cures Act now mandates standardized FHIR APIs for all certified EHR users, covering patient and population data exchange. The CMS-0057-F rule expands that mandate to regulated payers with a cutoff of January 2027. Engineering teams that are not on FHIR R4 are already behind.
Why FHIR Is Transforming Healthcare?
Healthcare has been on HL7 v2 for decades. Messages passed between isolated systems, fax machines carried lab results to people who typed the same data into another system, and EHR vendors had no financial incentive to ensure any of it interoperated cleanly. A patient moving from one care setting to another meant a data gap, every single time.
FHIR changes the model. With the HL7 FHIR R5 specification, health data becomes RESTful, JSON-based resources that any authorized system can query directly. A patient record is its own endpoint. A lab result is its own endpoint. No proprietary connectors. No manual re-entry.
Understanding FHIR Resources
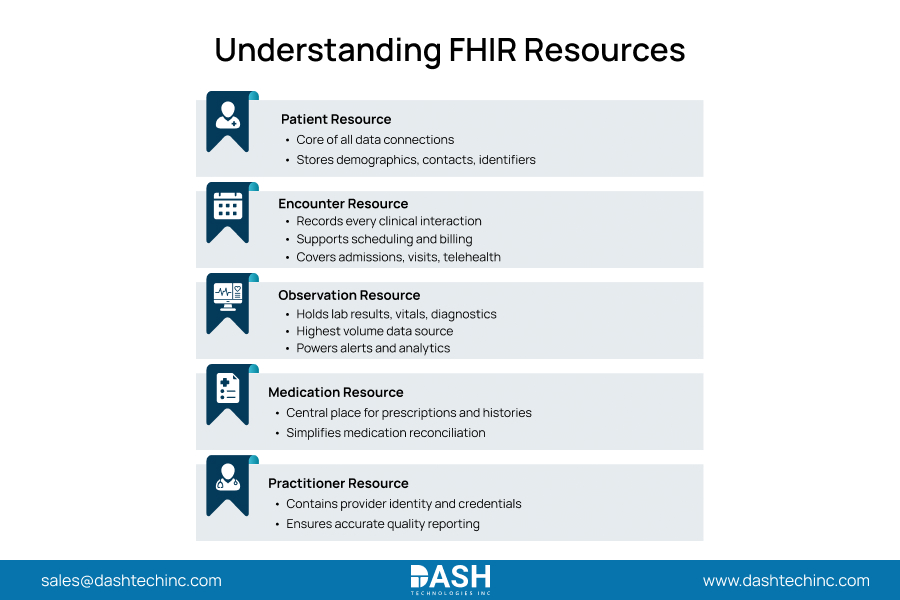
FHIR structures data into resources. Think of each one as a self-contained data object with its own endpoint. Five of them appear in virtually every production clinical application.
- Patient Resource
The Patient resource is the anchor. Demographic identifiers, contact details, record linkages: if you skip it, nothing else in your implementation connects. - Encounter Resource
Every clinical interaction connects to this endpoint. Covering the entire care lifecycle, from pre-admission to discharge. This includes inpatient stays, ER visits, telehealth, and outpatient appointments. Encounter data strictly drives scheduling engines and billing workflows. Engineering teams architecting clinical documentation rely entirely on this core resource. - Observation Resource
Lab results, vital signs, point-of-care measurements, diagnostic readings: all of it goes in Observation. It’s the highest-volume resource in any production system and the one your alerting, monitoring, and analytics pipelines pull from most. - Medication Resource
Every transition of care with HL7 v2 data means manual medication reconciliation. The Medication resource puts prescriptions, histories, and administration records in one queryable place. - Practitioner Resource
Provider identity, credentials, and role. Implement it correctly, and attribution in quality reports just works. Miss it, and you’re chasing data gaps after the fact.
FHIR API Architecture Explained
An application sends an HTTPS request to the FHIR server. The server validates it against R4/R5, queries the EHR or clinical data store, and returns structured JSON. SMART on FHIR intercepts each request at the gateway for authorization before any data flows.
Full Chain: Application → FHIR API → EHR → Healthcare Data.
This architecture eliminates vendor lock-in. Applications conforming to FHIR R4 work across Epic, Cerner, and Meditech without a separate integration project per vendor or contract renegotiations every time a health system switches EHR platforms.
SMART on FHIR Explained
SMART on FHIR runs on OAuth 2.0 and OpenID Connect. OAuth 2.0 handles authorization. OpenID Connect tokens verify both the end user and the application before any data moves. After authentication, access gets scoped to a specific patient or resource set, nothing broader.
EHR-initiated sessions pass patient context at launch; standalone launches come from outside the EHR. One application, both modes. Patient apps read their own records, analytics platforms get population-level access, and neither gets more than its explicit grant allows. Every application that stores or transmits PHI runs under SMART on FHIR. No exceptions.
Step-by-Step FHIR Development Process
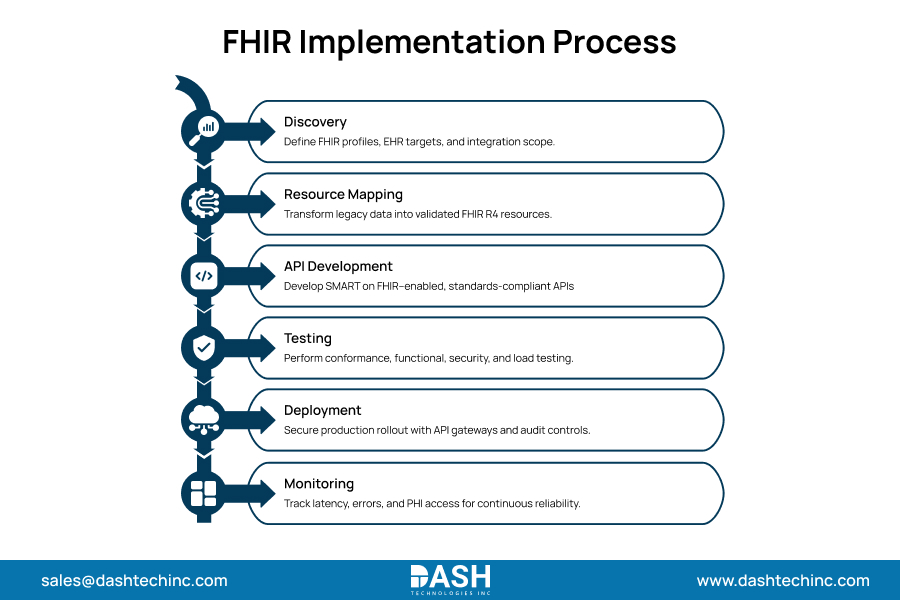
- Discovery
Three things the team needs before writing a line of code: which FHIR profiles apply to this use case (US Core, USCDI, or specialty-specific), which EHR implementations to target, and what each vendor’s sandbox actually exposes versus what their docs say it does. That last one usually surprises people. The gap between vendor documentation and sandbox reality is where discovery earns its budget. - Resource Mapping
Translate legacy data models like HL7 v2, CDA, and proprietary schemas into FHIR R4 resource structures. Then, validate each mapping using HL7 conformance tools. Wrong mappings corrupt clinical records. A documented, validated mapping schema is what separates a production system from a prototype that breaks in the second hospital. - API Development
HAPI FHIR and managed cloud services, Google Cloud Healthcare API, Azure Health Data Services, AWS HealthLake, are the standard build choices. SMART on FHIR authorization goes in at day one. Teams that retrofit it later reliably break integrations and open compliance gaps in the same move. - Testing
Run the HL7 FHIR validator against every resource type, load test under production-scale volumes, and confirm SMART flows work in both EHR-launched and standalone modes. Nothing ships before that’s done. - Deployment
Behind a managed gateway: rate limiting, TLS 1.2+ enforcement, and audit logging from the first request. - Monitoring
PHI access logging is not optional under HIPAA. Track latency and error rates by resource type; a spike in Observation errors at 2 am is a clinical pipeline failure, not background noise.
Most Common FHIR Use Cases
- Patient Apps:
Via the CMS-0057-F-mandated Patient Access API; portals and mobile applications give patients direct access to their FHIR-structured records, including appointment histories, lab results, and medication lists. Regulated payers are already required to have this. - Telehealth:
Encounter and Observation resources feed directly into virtual visit workflows. Providers see complete records without toggling between systems. That duplicate data-entry problem from early telehealth is an architecture problem, not a clinical one, and FHIR solves it at the source. - Remote Patient Monitoring (RPM):
IoT device output maps to the Observation resource. Continuous home monitoring feeds flow into alerting systems in real time, with no manual collection step in between. - Population Health:
Bulk FHIR data access pulls Patient, Condition, and Observation records across entire populations. Risk stratification models and quality reporting workflows that depend on longitudinal data finally get the foundation they need. - Provider Dashboards:
Service-line administrators get cohort views, care gap alerts, and operational metrics through FHIR-connected analytics. The alternative is hours-old manual exports from disconnected EHR reports.
Best Practices
- API Governance:
Before the first external call, publish a version policy. Share a timeline for deprecation. Clearly state backward-compatibility commitments. External teams will build integrations around those commitments. Undocumented breaking changes don’t just break integrations; they break the relationships behind them. - Security Controls:
Administrative pipelines require strict MFA, tightly scoped OAuth 2.0 parameters, and automated credential rotation. CMS-0057-F mandates these exact mechanisms as the absolute compliance baseline. - Documentation:
The API ships with a machine-readable FHIR capability statement. It also includes detailed, human-readable integration docs. Both should be available right at deployment. Undocumented APIs expose you to ONC information blocking enforcement. That’s an active compliance risk, not a best practice recommendation. - Version Management:
Build resource transformation logic capable of handling version migration without breaking integrations; the teams that skip this step are the ones scrambling when the next upgrade cycle hits.
Build FHIR-Powered Healthcare Applications
FHIR API development has stopped being optional for years. The compliance clock runs through 2027, and the enforcement mechanisms are already in place. Hospital executives who build FHIR-compliant architecture now don’t just satisfy a mandate. They permanently retire the integration debt that has paralyzed healthcare data exchange for thirty years.
Our interoperability engineering teams design and deploy production FHIR API solutions across hospital service lines: Cardiology, Radiology, Orthopedics, and beyond. Connect with us to build the FHIR infrastructure your clinical applications demand.
Frequently Asked Questions
About Dash
Dash Technologies Inc.
We’re technology experts with a passion for bringing concepts to life. By leveraging a unique, consultative process and an agile development approach, we translate business challenges into technology solutions Get in touch.