
Cerner EHR Integration: APIs, Challenges, Cost, and Best Practices
hen hospital IT says they’re “connecting to Cerner,” they usually mean one workflow. Cerner EHR integration is actually five protocol layers running in parallel, each with different requirements; all live at the same time. Oracle Health’s $28.3 billion acquisition of Cerner in 2022 didn’t clean this up. It put a cloud migration deadline on top of a version management problem that was already there.
With Oracle Health holding roughly 23% of the acute care EHR market, health systems don’t get to wait for Oracle to simplify the picture. Oracle Cerner integration must work as-is, across all five layers, while Oracle is actively rebuilding the foundation underneath.
What Is Cerner EHR Integration?
Most teams scope it too narrowly. Cerner EHR integration is the plumbing between Oracle Health EHR (formerly Cerner Millennium) and everything else a health system runs: clinical tools, billing platforms, remote monitoring devices, and analytics engines. All of them need a live data connection into Cerner, and that connection isn’t one thing.
Real EHR and EMR integration is not just moving data. It makes that data usable when a clinician actually needs it.
Common Cerner Integration Use Cases
Where health systems feel the gap most:
- Telehealth: Without a live integration, virtual encounter data, vitals, and session notes don’t land on the patient’s record. Clinicians document twice. The data disappears.
- Patient portal: They run on FHIR R4. Scheduling, secure messaging, and records of access all depend on it. The ONC’s Cures Act Final Rule requires patient-facing API access. If this layer isn’t built, the health system is out of compliance.
- Remote monitoring: Data doesn’t flow anywhere without a live connection. Glucose readings, cardiac telemetry, wearable vitals: someone re-enters it by hand, or it disappears.
- Revenue cycle: Billing accuracy requires direct access to diagnosis codes and charge data as they’re generated. Every manual handoff is another place for the numbers to drift.
- CDS Hooks: Can only fire at chart open or order entry when the integration is live. Without it, that decision of support never reaches the clinician at the moment they need it.
Cerner Integration Technologies
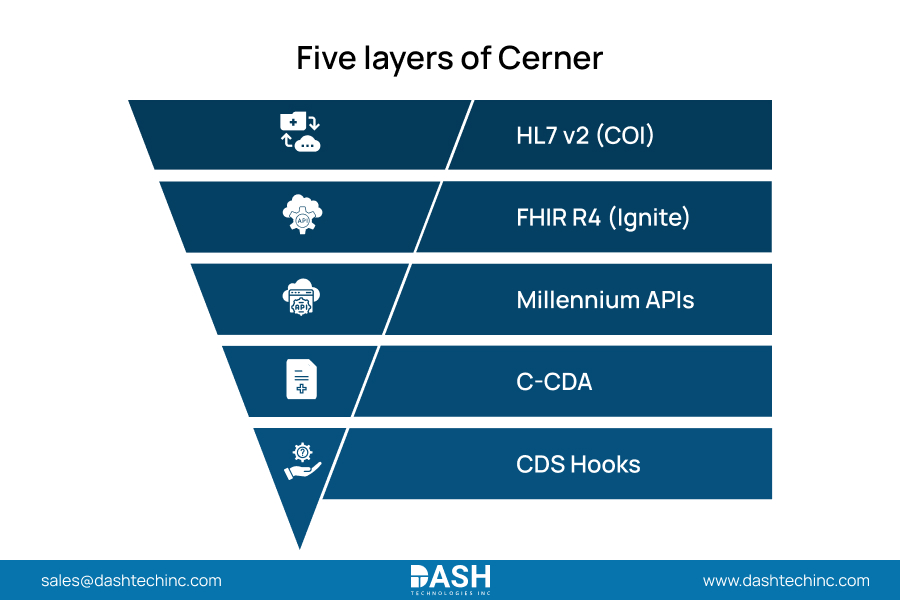
Five layers every Cerner API integration must handle:
| Protocol | Primary Use | Key Consideration |
| HL7 v2 (COI) | ADT events, lab orders, and scheduling | High-volume; most operationally tested path |
| FHIR R4 (Ignite) | Patient portals, SMART on FHIR apps | Cerner FHIR API requires OAuth 2.0; DSTU-2 is retiring |
| Millennium APIs | Specialty scheduling, custom workflows | Tightly coupled to Cerner’s internal data model |
| C-CDA | Discharge summaries, referral packets | Structured document exchange |
| CDS Hooks | Clinical decision support | Fires inside EHR at chart open or order entry |
SMART on FHIR apps require a context switch: the clinician leaves Cerner to use the external tool. In time-critical situations, the handoff breaks real workflows. Millennium APIs create a different risk: tight coupling to Cerner’s internal data model means every platform version change is a potential production incident without active lifecycle management.
Top Cerner Integration Challenges
-
Data Mapping
Start here because most teams don’t. The API work is visible. Data quality problems stay invisible until they show up as clinical decision errors at go-live.
Health systems carry decades of records across systems with no shared convention for terminology, structure, or coding. Normalizing all of that to SNOMED CT, LOINC, and RxNorm, then aligning it to Cerner’s data model, is architecture work. Teams that scope it wrong don’t find out until something clinical breaks. -
Legacy Infrastructure
Most health systems don’t start from a clean slate. Existing integrations run on older HL7 v2 pipes, vendor middleware that hasn’t been updated in years, and Millennium API connections tied to versions Oracle has already moved past. Any Cerner integration project that doesn’t account for what’s already running will break it.
-
API Version Drift
Oracle ships platform updates on a continuous cycle. Integrations working on a particular endpoint version don’t get a grace period when that version is deprecated. They just stop working, usually in production, usually without advance notice. Version management is an ongoing operational discipline, not a task you complete and move on from.
-
Security and HIPAA Compliance
Security failures in Cerner integrations come from gaps in enforcement, not knowledge. OAuth 2.0, TLS 1.2 minimum, role-based access controls, audit logging on every PHI access event: the checklist is short. Holding to it through a build under deadline pressure is the problem.
Access creep is the practical failure mode. A billing system picks up write access to clinical notes during a sprint focused on charge capture, not permissions. A compliance audit eighteen months later is where it surfaces. Fixing the access model then costs far more than getting it right during the build. -
Workflow Disruption
Technically correct integration can be clinically useless. Messages are transmitted, fields are populated, and the care team doesn’t use the workflow because the alert logic doesn’t match how they operate. You find that out by running the integration past actual clinicians before go-live, not after.
-
Scalability
Single-system integrations that weren’t designed for enterprise load become production risks as health systems add data sources, users, and connected applications. An architecture that works for one hospital doesn’t automatically hold across a multi-site system. Scalability has to be designed, not retrofitted.
Cerner Integration Cost Factors
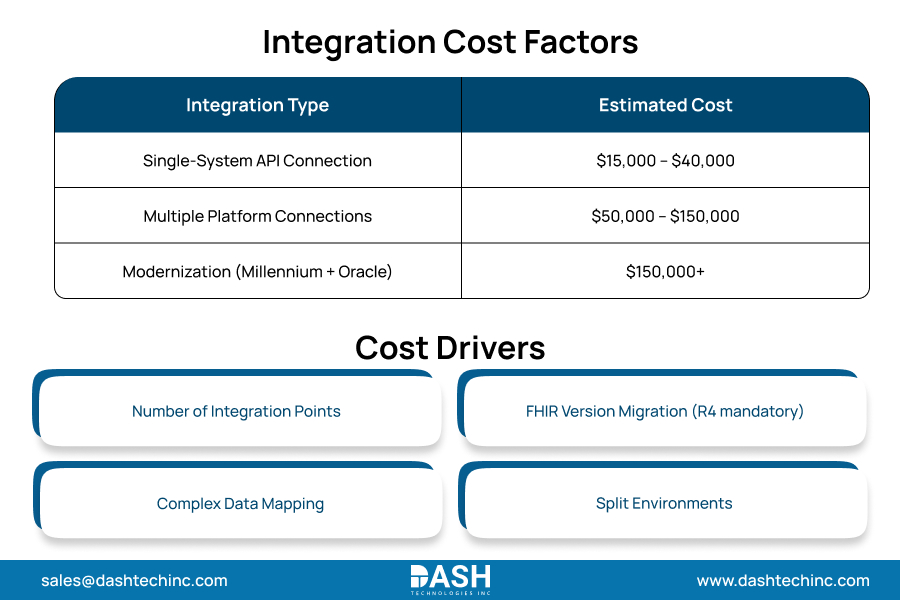
Budget surprises come from underestimating the scope. A single-system API connection runs $15,000 to $40,000. Connecting multiple platforms pushes that to $50,000 to $150,000. Modernization projects straddling the Millennium and Oracle Health Cloud routinely clear to $150,000.
Several factors push projects toward the higher end: more integration points, FHIR version migration (Oracle’s DSTU-2 retirement makes R4 mandatory for connected systems), heavier data mapping, and split environments. Health systems running multiple Cerner integration services should be built as a unified platform. The project-by-project approach generates rework that compounds fast.
Cerner Integration Best Practices
Six rules that hold across every implementation:
- Use versioned API contracts, not direct connections to internal states. Platform states change. Everything built against an internal state break when the platform moves.
- Migrate to FHIR R4 now. Oracle is retiring from DSTU-2. The question isn’t whether to migrate. It’s whether it happens on a planned timeline or in response to a production incident.
- Data governance is architectural work. Terminology normalization and clinical data validation belong in the design phase, not post-launch.
- Test environments need to match production on security controls, data volume, and API version. A stub catches easy bugs. The defects that matter turn up at go-live.
- Run clinical validation before deployment. Technical correctness and clinical utility are separate tests. Both have to be cleared.
- Own version management as ongoing operations. Oracle’s update cycle doesn’t pause for live integrations.
How DASH Helps
DASH’s healthcare interoperability services cover Cerner across the full protocol stack: HL7 v2, FHIR R4, Millennium APIs. Data mapping, security architecture, and clinical workflow validation go into every engagement from the start, not as corrections when something breaks in production.
Most Cerner integration failures are preventable. They happen because teams treat data mapping as cleanup, skip real test environments, or don’t involve clinicians until after deployment. DASH structures engagements to catch those problems before they become go-live incidents. If you’re starting one or fixing one that’s drifted, contact Dashtech.
Frequently Asked Questions
About Dash
Dash Technologies Inc.
We’re technology experts with a passion for bringing concepts to life. By leveraging a unique, consultative process and an agile development approach, we translate business challenges into technology solutions Get in touch.






