
Clinical Data Integration: Connecting Trial, Lab, and Real-World Data
Clinical data integration is where most health systems are quietly losing ground. Clinical data integration is where most health systems are quietly losing ground. Not because they lack data, but because the data they have doesn’t connect. Trials in one system, labs in another, EHR records in a third, claims somewhere else entirely. And the research cycle takes years longer than science requires. That is an architecture problem, and it compounds every quarter it goes unaddressed.
Why Fragmented Clinical Data Costs More Than Organizations Realize?
Data silos don’t just slow research but also distort it. The costs show up at every layer of the research and care cycle:
- Protocol adjustments that should take days stretch to weeks
- Patient matching for trials runs against partial clinical pictures
- Outcomes measurement fails at the reporting layer, even when clinical performance is strong
The regulatory dimension is direct. The Office of the National Coordinator for Health Information Technology has made healthcare interoperability a federal priority, with information blocking rules carrying real penalties. Fragmented architecture puts health systems at compliance risk that often doesn’t surface until an audit.
Healthcare data integration failures compound that risk. Value-based contracts require precision at the population level. Disconnected data doesn’t produce it.
Sources of Clinical Data That Health Systems Must Integrate
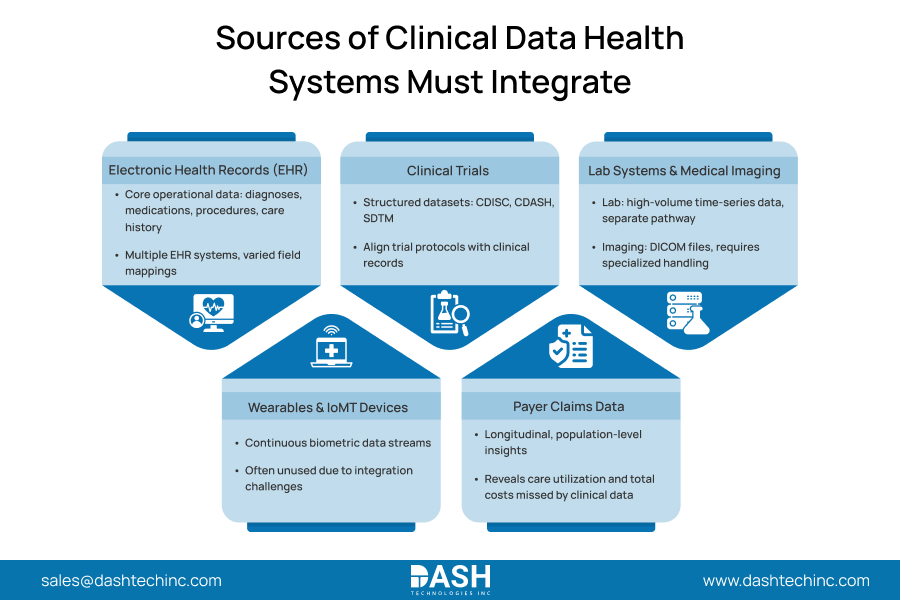
The challenge isn’t a single integration problem. It’s six overlapping ones.
- Electronic Health Records
EHR databases keep key information. They list patient diagnoses. They show current medications. They also include clinical procedures and treatment of histories. This data often covers many instances in one enterprise. This leads to fragmented field mappings. - Clinical Trials
Trial environments execute exclusively on CDISC, CDASH, and SDTM-structured datasets. Core clinical data management strictly requires bridging this architectural junction, mapping rigid trial protocols directly against raw operational patient records. - Lab Systems and Medical Imaging
Lab systems sit outside the main EHR data flow and produce high-volume time-series data that needs its own integration path. Medical Imaging generates DICOM files requiring specialized infrastructure. Imaging AI can’t function unless the organization surfaces that data alongside clinical context. - Wearables and IoMT
Wearables and IoMT devices produce continuous biometric streams that most organizations can’t yet ingest, leaving real-world evidence from those devices unused. - Payer Claims Data
Payer claims data is the only source that gives you a longitudinal, population-level view. EHR records and trial data don’t get there. Claims surface utilization patterns and total cost of care across settings that clinical records miss.
Struggling to Connect Trial, Lab, and Real-World Data?
Our healthcare interoperability specialists help you streamline data exchange, improve data consistency, and create a connected research ecosystem.
Connect With Our AI ExpertsWhat Integration Actually Delivers?
- Research Timeline Compression
Research data integration compresses timelines when trial data, lab results, and real-world evidence run on shared infrastructure. Eligibility criteria for trial matching get evaluated against complete records, not fragments. - Value-Based Care Performance
Value-based care reporting depends on this. CMS quality performance measurement requires longitudinal, multi-source records. Organizations running disconnected data fail at the reporting layer regardless of how well their clinicians perform. - Operational Efficiency
The efficiency gains are real, too. Clinicians spending their time reconciling results across three systems aren’t spending that time on care. Integration eliminates that burden at the workflow level, not through workarounds.
Integration Technologies That Make It Work
- HL7 FHIR R4
HL7 FHIR R5 dictates the API structures and exchange protocols at the standards layer. This architecture lets different vendor systems share clinical data directly. It skips the need for custom point-to-point integrations. Are your environments still running legacy HL7 v2 feeds? The industry is moving past that architecture, and the gap grows with every new implementation guide to update. Healthcare interoperability at scale runs through FHIR, not around it. Event-driven API connections replace batch transfers, getting data to the right place when it’s needed. - ETL Pipelines
ETL pipelines extract from source systems, apply standardization logic, and load structured records into target repositories. That sounds mechanical. In practice, the quality of that design is what separates trustworthy integrated data from centralized noise. - Clinical Data Lake
A well-designed clinical data lake puts all of it—trial data, EHR records, claims, lab results, and device streams, behind a single query interface. That’s the difference between real-world data integration as a research capability and real-world data integration as a compliance obligation.
Key Challenges in Clinical Data Integration
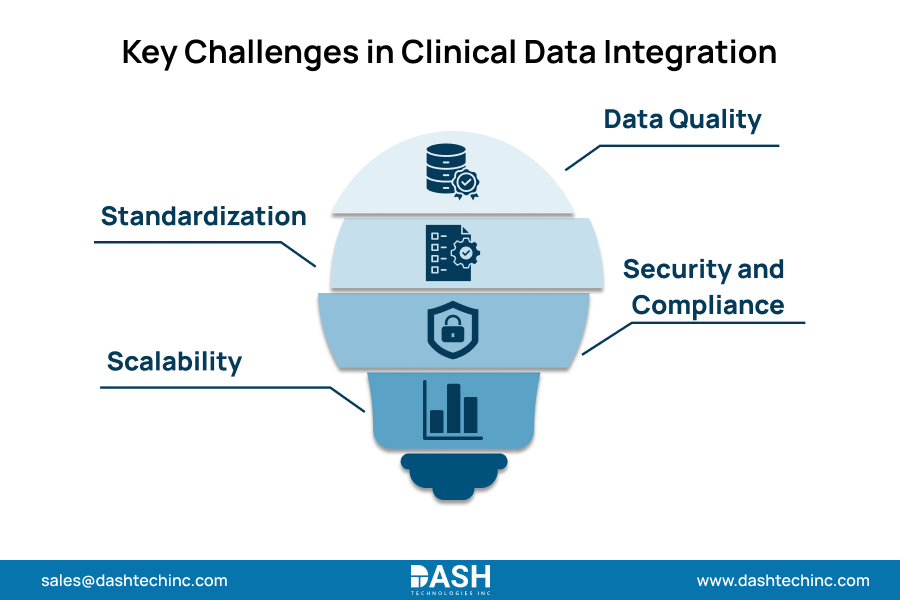
- Data Quality
Data quality is the first barrier. Duplicate records, inconsistent terminology, missing values, and fields that mean different things across facilities: no integration architecture fixes upstream quality problems automatically. Organizations that skip data quality investment get centralized garbage, not centralized insight. - Standardization
Standardization requires clinical informatics expertise, not just technical skill. SNOMED CT, LOINC, RxNorm, and ICD codes all appear across clinical records in inconsistent forms. Mapping them to consistent representations across sources is the clinical data management work that determines whether integrated data is usable for research. - Security and Compliance
Every system brought into an integrated environment adds to the attack surface. HIPAA protections for individually identifiable health information don’t get easier to implement as environments grow. De-identification pipelines, access controls, and audit logging belong in the architecture from day one. - Scalability
Pilot-scale architecture breaks under production load. Add EHR records for hundreds of thousands of patients, continuous device streams, and imaging archives, and the infrastructure that worked during a proof of concept fails in ways it didn’t during testing.
Best Practices for Clinical Data Integration Programs
- Governance Before Go-Live
Get governance in place before the integration goes live. Ownership, access approval, quality escalation paths, lineage documentation: these need answers before the first data starts moving. - Master Data Management
Master data management is what lets records from different systems actually join. Common patient, provider, and facility identifiers don’t happen by default. - Data Harmonization
Data harmonization applies consistent terminology, units, and coding standards before data enters the shared infrastructure. It is clinical informatics work that makes integrated data analytically useful rather than structurally unified but semantically inconsistent. - Security Architecture
Security architecture requires the same rigor as integration architecture. Healthcare providers working with Dashtech on data infrastructure embed security controls at the pipeline level, not as a layer retrofitted after integration is complete.
The Direction Clinical Data Integration Is Heading
- AI-Augmented Research
AI-augmented research cannot function without integrated data. Machine learning models for trial candidate identification, outcome prediction, and real-world safety signal detection all need unified, validated, longitudinal records as their input. - Real-Time Evidence Generation
Real-time evidence generation is not a research concept anymore. Health systems that surface outcomes data continuously can adjust protocols and catch safety signals well before organizations running quarterly extracts even know there is something to investigate. - Federated Data Models
Federated data models solve problems that centralized architectures cannot. They let organizations run multi-site research data integration without moving protected health information into a shared repository. Analyses run across distributed datasets locally, with only aggregate results leaving each site. Healthcare data integration executed at this scale does not just improve research throughput. It changes what research questions health systems can ask.
Conclusion
Clinical data integration determines whether health systems generate insight or generate archives. The gap widens with every research cycle, value-based contract, and AI capability that integrated data makes possible.
We build clinical data integration infrastructure across the full range of provider environments: EHR interoperability, FHIR API implementation, data lake architecture, and research data pipelines. Contact us to build a connected clinical data infrastructure that your organization actually owns.
Frequently Asked Questions
About Dash
Dash Technologies Inc.
We’re technology experts with a passion for bringing concepts to life. By leveraging a unique, consultative process and an agile development approach, we translate business challenges into technology solutions Get in touch.





