Remote Patient Monitoring (RPM): Implementation Challenges and Best Practices
Remote patient monitoring programs fail at implementation, not at concept. The devices ship, and the data flows. Then the real problem surfaces: the EHR rejects the format; alerts have no routing logic, and the care team has no workflow built around any of it. RPM implementation treated as a procurement decision hits that wall at go-live. That lesson costs more than proper planning would have.
The clinical case for continuous monitoring in high-risk populations is documented. So is the revenue case under CMS chronic care reimbursement. The gap between buying devices and running a program is where most organizations get stuck. That gap is an infrastructure problem, not a clinical one.
Most programs that stall do not fail because the clinical team rejected RPM. They stall because nobody built the plumbing. EHR integration, alert logic, workflow design; all of it must be in place before the first device leaves the warehouse. Organizations that figure that out before go-live run programs. The ones that figure it out after running post-mortems.
Why RPM Adoption Is Accelerating?
CMS expanded reimbursement for remote patient monitoring under chronic care management codes. Connected care systems capturing blood pressure, glucose, weight, and SpO2 now generate billable clinical data between visits. The financial model changed. Programs pay for themselves when coded correctly, and patient compliance holds.
Value-based care contracts reinforced the clinical case. Providers accountable for the total cost of care need visibility into high-risk patients between visits. Remote patient monitoring is the infrastructure that makes proactive intervention possible at scale. Without it, the team reacts to hospitalization. With it, they prevent them.
The billing structure rewards compliance. CPT codes 99453 and 99454 cover device setup and supply. 99457 and 99458 cover the monthly treatment management time. A high-risk population generating compliant data and billing correctly offsets the infrastructure investment in a very short time. That is, before the cost avoidance from reduced hospitalizations is counted.
Turn RPM Data into Better Outcomes
Enable scalable remote patient monitoring with connected digital health solutions built for proactive care delivery, compliance, and operational efficiency.
Talk to Our ExpertsCore Components of an RPM Ecosystem
Every functional RPM platform runs on four layers:
- Device layer: Patient monitoring devices that capture the biometric signal: weight, BP, glucose, SpO2
- Transmission layer: Cellular or WiFi connectivity, moving readings from device to platform
- Analytics layer: Threshold logic and trend detection that converts raw data into clinical signals
- Alert layer: Routing rules that send the right signal to the right care team member
RPM platforms that skip EHR integration produce a second data silo. Remote care platforms without alert routing to produce noise. Patient monitoring systems running outside clinical workflows are equipment. Not all programs.
The device layer without the transmission layer is a standalone monitor. The transmission layer without the analytics layer is a data dump. The analytics layer without the alert layer is a report nobody reads. Each layer connects to the next one, or the data stops mattering before it reaches a clinician.
Common RPM Implementation Challenges
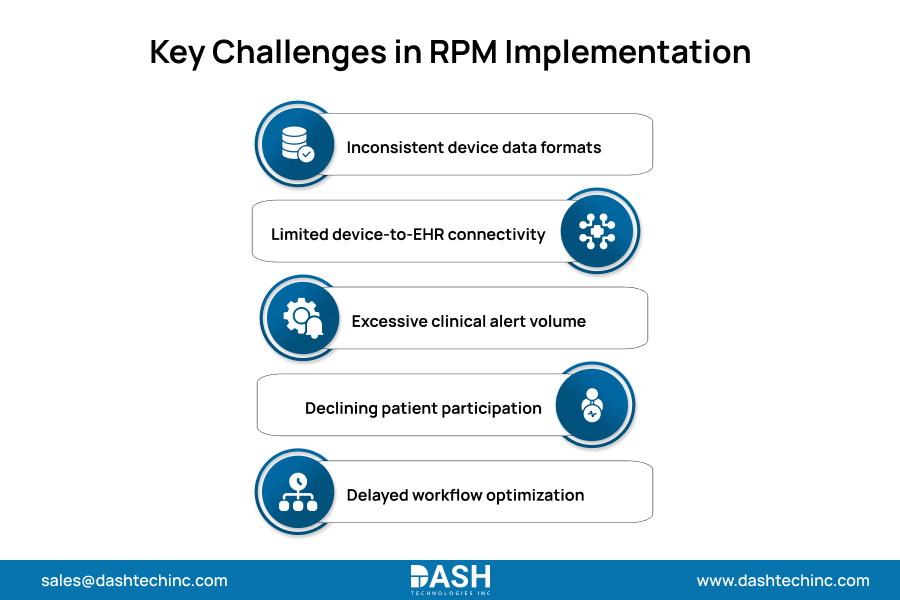
RPM integration challenges show up in four places consistently:
- Data format inconsistency: Devices transmit in proprietary protocols requiring translation before EHR ingestion
- Healthcare device interoperability gaps: Monitoring data and clinical data sit in separate systems with no automated bridge
- Alert fatigue: Unfiltered data generates clinical noise that care teams learn to ignore
- Patient engagement drop-off: Compliance collapses after the first 30 days without structured onboarding
Each one has a fix. None of them resolve their post-launch. Programs that survive the first 90 days addressed these before the first device shipped.
Alert fatigue ends programs quietly. Unfiltered threshold alerts across a 300-patient population generate hundreds of notifications per day. Care teams adapt by ignoring them. The fix is threshold calibration before launching. Not after the team has already learned to tune out the noise.
Role of Interoperability in RPM Success
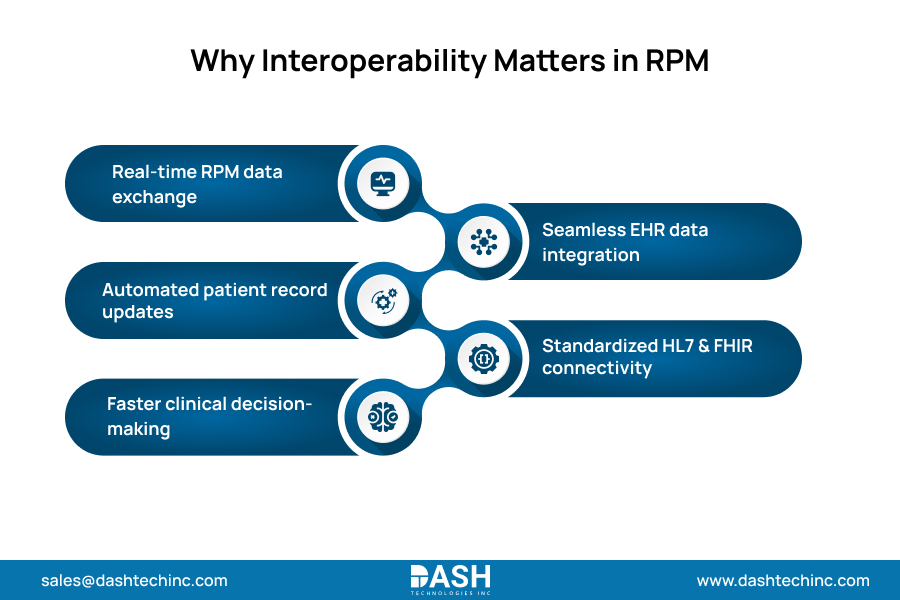
Connected healthcare devices generate data. Interoperability determines whether that data reaches the clinician in time to matter.
FHIR-based RPM data integration writes monitoring readings directly into the patient’s record without manual entry. Care plans update from monitoring trends. HL7 and FHIR provide the technical standard. The friction is in execution: EHR vendors, device manufacturers, and RPM platform vendors run on different integration schedules. Organizations that skip interoperability requirements in the platform selection process find the gaps after contract signature. Not before.
The execution gap comes down to timing. EHR vendors push API updates on their own schedules. Device manufacturers certify specific firmware versions. RPM platform vendors release integration updates quarterly. Getting all three aligned is a project management problem as much as a technical one. Organizations that put interoperability requirements in the contract before signature avoid paying for that alignment after the fact.
Best Practices for Scaling RPM Programs
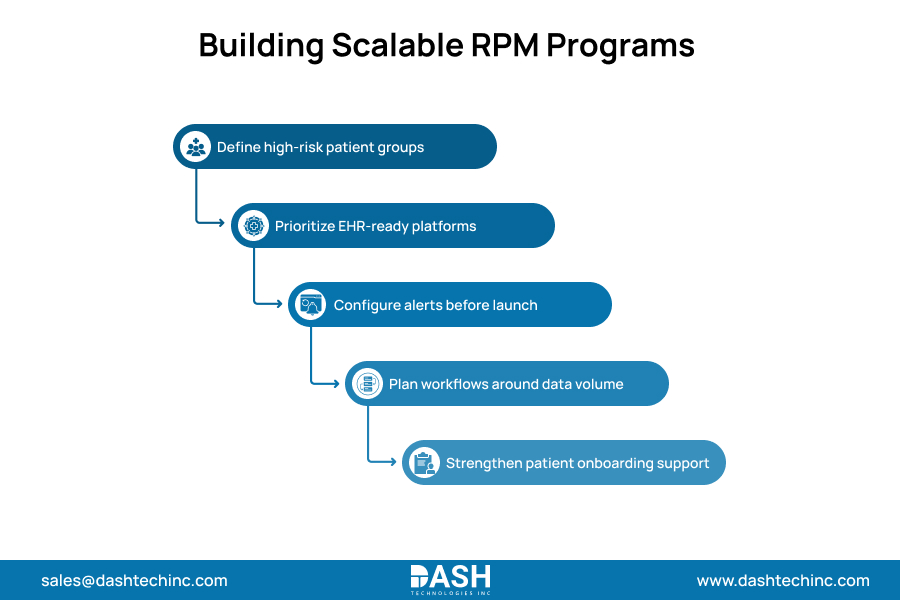
Scalable RPM infrastructure starts with platform selection. Not device selection. The sequence that works:
- Define the patient population first: high-risk chronic patients with measurable biometric signals between visits
- Choose the platform on EHR integration capability and alert configurability, not device aesthetics
- Set alert thresholds before launch, not after 90 days of noise have trained the team to ignore them
- Build care team workflows around monitoring volume before devices go out
- Treat patient onboarding and technical support as infrastructure, not something you overlook afterwards
RPM best practices that scale share one thing: all the above run before the first patient receives a device. Virtual care strategy shapes which population enters the program. Start where the clinical and financial case is clear.
Population definition is the anchor; RPM works best where a clear biometric signal exists between visits, and a defined intervention follows when it triggers. Heart failure, COPD, hypertension, and diabetes fit that model. Broad deployment without that specificity generates data volume with no clear clinical action attached.
How RPM Supports Preventive and Chronic Care?
Chronic care management programs that include RPM change when the team acts. A heart failure patient with a rising weight trend gets a call before hospitalization. Preventive healthcare analytics built on monitoring data find population-level signals that visit-based care never sees.
The patient moving toward uncontrolled hypertension appears in a monitoring report before the ED visit. That is a structural shift in intervention timing. Earlier action means more options.
COPD patients with daily SpO2 tracking get escalated before saturation drops into an emergency range. Diabetic patients with continuous glucose integration surface control problems weeks before the next A1C visit. Heart failure and COPD are where RPM delivers its clearest financial return. Our cardiac RPM infrastructure connects monitoring data directly into cardiology workflows with the threshold logic and alert routing that those programs require.
Conclusion
The programs that scale are not more complex than the ones that collapse at go-live. They are better sequenced. Infrastructure before devices, and better workflow design before they go live. Threshold calibration before the first alert fires. That sequence is not complicated. It is the step most organizations skip because procurement moved faster than planning.
RPM programs that scale run on connected infrastructure, EHR integration, and clinical workflows designed to monitor data from day one. Device procurement without platform integration produces data no one acts on. Our provider engineering team builds RPM platforms, integration layers, and connected care infrastructure for provider organizations at every stage of program maturity.
If your organization is ready to build a scalable RPM program, our team starts with the integration architecture, not the device catalog.
Frequently Asked Questions
About Dash
Dash Technologies Inc.
We’re technology experts with a passion for bringing concepts to life. By leveraging a unique, consultative process and an agile development approach, we translate business challenges into technology solutions Get in touch.