EHR Integration Strategies: Point-to-Point vs API vs Middleware
EHR integration strategies dictate exactly what a hospital’s data infrastructure actually delivers. Theoretical performance remains irrelevant. Real execution occurs during critical clinical moments when live lab results must reach physicians before operational decisions happen. The underlying architecture either scales or fails completely.
Organizations locked into flawed architectural models pay severe operational penalties. They suffer compounding software costs, unmanaged clinical risk, constant staff inefficiencies, and completely untrustworthy analytics outputs. Most executives only recognize this catastrophic structural failure years after deployment.
Why EHR Integration Is Critical for Modern Healthcare?
EHR interoperability is the operational backbone. Lab platforms, radiology tools, patient portals, revenue cycle engines, connected devices: they all depend on data arriving correctly and on time. Healthcare system integration is what keeps those feeds accurate and clinically usable. When it fragments, everything built on top inherits the problem.
When it breaks down, the consequences are immediate. Clinicians make decisions from incomplete records. Staff compensate through emails and manual re-entry. A 2022 study in JAMA Network Open identified poor data integration as a primary barrier to clinical decision support across health systems. AI initiatives, population health programs, and analytics investments all of them inherit that fragmentation directly.
Hospital integration strategy means treating data exchange as infrastructure. Not a project with a finish line. Every architectural decision made today constrains what AI initiatives, population health programs, and analytics investments can do five years out. CIOs who frame this as a finite build find out why that framing is wrong, usually at the worst possible time.
Common EHR Integration Challenges Hospitals Face
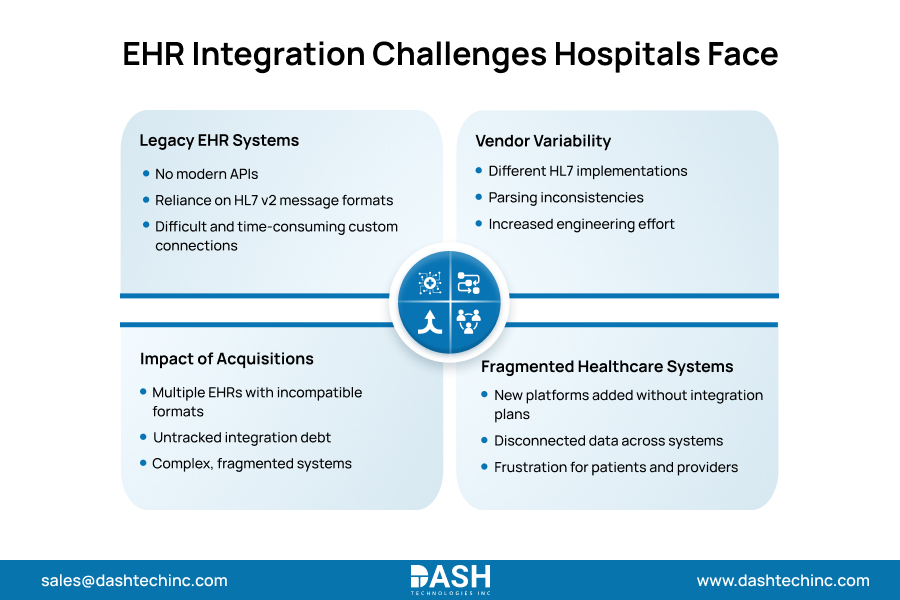
Every health system runs into the same healthcare integration challenges. Legacy EHRs expose no modern APIs. That forces custom connections built on HL7 v2 message formats, formats that were never designed for interoperability at scale. Getting those to parse reliably across different vendor implementations takes far more engineering time than most IT roadmaps account for. The cost only becomes visible after the team is already committed.
Acquisitions compound this fast. Every merged practice arrives with its own EHR, format assumptions that match nothing else in the environment, and integration of debt nobody fully inventoried before the deal closed. Fragmented healthcare systems are not relics. They regenerate, with every acquisition; every new platform dropped into the stack without a clear plan for connecting it.
The result: they inherit entirely new sets of incompatible software, compounding the complexity and creating a fragile web of disconnected data that frustrates both patients and providers.
Understanding Point-to-Point Integration
Point-to-point integration in healthcare connects two systems directly. One source, one translation layer, one destination. Nothing in between.
Benefits
- It deploys fast.
- No middleware platform required upfront.
- For small organizations managing two or three systems that need to communicate, direct EHR integration is often the right starting point.
- When a hospital only needs two specific applications to share a limited dataset, a direct connection is often the path of least resistance.
Limitations
- Ten systems connected point-to-point require up to 45 separate connections.
- Each needs independent maintenance, monitoring, and version management whenever either endpoint changes its data model.
- At that volume, it stops being a data strategy and becomes an engineering liability.
- It compounds with every system added.
- Teams that start here routinely find themselves three years later managing a web of custom feeds with no clean path out.
Choose the Right EHR Integration Strategy
From legacy systems to FHIR APIs, we help healthcare organizations design integration strategies that work.
Talk to an ExpertAPI-Based Integration in Healthcare
FHIR APIs changed what modern healthcare interoperability looks like in practice. No more custom one-off feeds for every connection. Healthcare API integration routes data through standardized endpoints built on the HL7 FHIR R4 specification, and any authorized system hits the same interface, regardless of what is running behind it.
Benefits of API-First Architecture
CMS’s Interoperability and Patient Access Rule mandated FHIR-based APIs for payer-to-provider data exchange. That set the regulatory floor. FHIR integration delivers real-time exchange without batch delays. And when a vendor gets replaced behind the API, the interface stays stable; modernization on one system does not cascade into reintegration work across everything connected to it.
Scalability Advantages
New systems join the same API layer. No new custom feeds. Vendor replacement becomes a backend swap; the interface stays stable whether the system behind it changes. Patient portals, analytics platforms, payer connections: all-consuming the same endpoints. The network is growing. The connection management burden does not exist.
Middleware-Based Integration Explained
Healthcare middleware handles what neither point-to-point connections nor APIs were built for. Format translation across HL7 v2, FHIR R4, DICOM, and proprietary schemas, happening simultaneously. Centralized routing, error handling at volume. A single governance layer across the entire environment, not separate monitoring scattered across dozens of individual feeds.
Integration Engines
Generic enterprise middleware was not built for clinical message volumes. ADT feeds, lab results, radiology orders, and pharmacy data, all processed at clinical scale, without degradation. Integration engine healthcare tools handle that specifically. Generic platforms do not. Without this layer, enterprise-scale data exchange is a planning document, not an operational reality.
Workflow Orchestration
A patient admission does not trigger one action. It triggers many: bed management, care team notifications, scheduling, and billing. Healthcare middleware orchestrates that chain. APIs handle individual requests between systems. They were not built to coordinate multi-step clinical workflows across departments. The gaps show up when a handoff fails at the wrong moment.
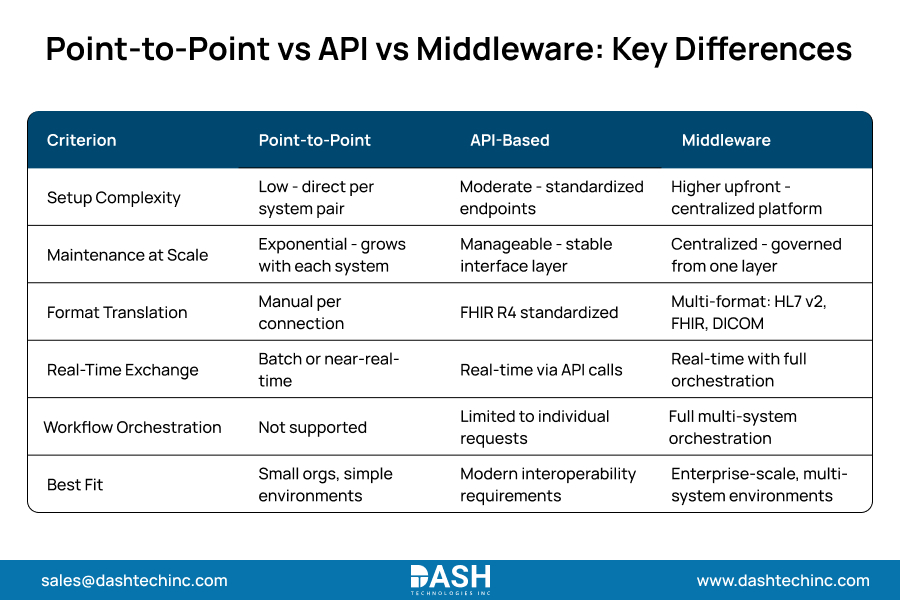
Point-to-Point vs API vs Middleware: Key Differences
This EHR integration comparison explains why most enterprise health systems end up deploying all three models as complementary layers within a single interoperability architecture.
How to Choose the Right EHR Integration Strategy?
Small organizations with a stable, limited system count can reasonably start with FHIR API connections and targeted direct EHR integration feeds. That holds, right up until an acquisition arrives, or the system count crosses the threshold where ungoverned connections start consuming IT capacity that was never allocated for it. Healthcare integration platform selection at that point is a governance decision. Not a speed one.
Past that threshold, the architecture needs FHIR API standardization paired with middleware-layer governance. Scalable EHR architecture absorbs new systems, new regulatory requirements, and new clinical use cases without forcing a full rearchitecture every time the stack shifts. That is not a premium target. It is the minimum requirement for any organization where the environment grows faster than the team can manually manage it.
Working with a team that operates at the healthcare interoperability infrastructure level separates an architecture that holds from one that demands a rebuild every time requirements shift. The decisions made at the design stage determine what is even possible three years from now.
Conclusion
Put plainly: point-to-point works in small, stable environments. It breaks under the scale. FHIR APIs set the standard for modern healthcare interoperability. Healthcare middleware handles what enterprise-level orchestration actually requires. At meaningful clinical volume, most health systems need all three, running as a governed stack, not as isolated choices made in different years by different teams.
The organizations that get this right are not picking between these models. They layer all three deliberately, each matched to what it actually does well, governed as a coherent architecture rather than stitched together as workarounds. Not because it looks clean on a whiteboard. Because it is the only configuration that holds under real clinical operating conditions.
Dashtech’s integration engineering team designs and builds layered architecture for health systems that need it working from day one.
About Dash
Dash Technologies Inc.
We’re technology experts with a passion for bringing concepts to life. By leveraging a unique, consultative process and an agile development approach, we translate business challenges into technology solutions Get in touch.