
Building a Scalable Virtual Care Infrastructure for Hospitals
The pandemic forced reactive telehealth deployments, leaving hospitals with highly fragmented IT environments. Operating isolated video tools alongside disconnected remote monitoring applications and aging EHR portals actively destroys clinical efficiency. These disparate digital touchpoints force medical staff to execute complex workarounds rather than streamlined care delivery.
Architecting true virtual care infrastructure requires a fundamental structural shift. It mandates a strictly governed foundation enabling care delivery across every setting and acuity level. Clinicians must never switch applications to execute medical interactions. Advanced virtual care platforms must consolidate scheduling, triage, clinical documentation, remote monitoring, and billing into connected capabilities operating on a singular shared data.
For hospital and health system leaders driving scalable digital health, selecting a basic telehealth vendor represents a profound strategic failure. The absolute executive mandate requires defining the exact architectural framework necessary to permanently embed virtual care directly into the core operational delivery model.
Limitations of Traditional Telehealth Models
First-generation telehealth deployments prioritized rapid implementation over enterprise scalability. These platforms secured immediate video access but completely ignored the rigorous operational integration required for sustainable care delivery. The resulting telehealth challenges actively paralyze health systems regardless of market size or geographical location.
- Clinical Workflow Isolation: Video platforms operating outside the EHR mandate massive documentation burdens. Forcing medical staff to manually transcribe notes and reconcile disparate records actively destroys the efficiency that virtual care promises.
- Fractured Patient Intelligence: Standalone systems process medical encounters as entirely isolated events. Denying virtual providers with immediate access to comprehensive longitudinal histories and chronic disease data guarantees dangerous clinical blind spots.
- Severe Revenue Leakage: Disconnected platforms cannot navigate complex billing codes, distinct state licensure rules, or rigid payer reimbursement requirements. This structural failure guarantees massive uncaptured revenue and generates unacceptable regulatory compliance exposure.
- High Acuity Execution Failures: Basic video tools completely collapse under the weight of advanced medical delivery. Executing remote ICU monitoring, post-surgical follow-up, and complex hospital-at-home programs demands rigorous clinical architecture rather than basic consumer-grade communication software.
What a Scalable Virtual Care Infrastructure Looks Like?
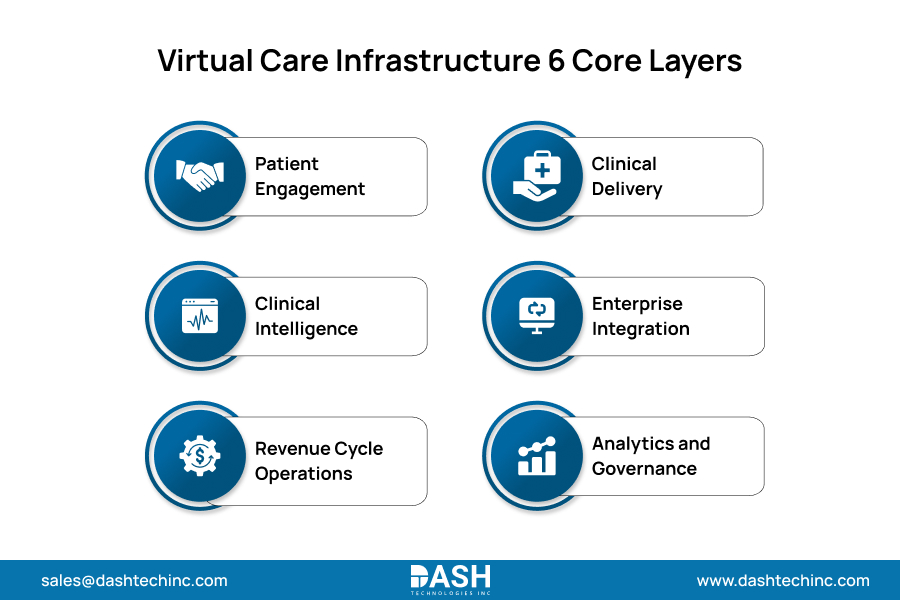
A production-grade virtual care infrastructure relies entirely on strict systemic integration rather than isolated technology deployments. Executing scalable digital health demands a rigorous healthcare platform architecture strictly organized across six core functional layers:
- Patient Engagement: Deploying frictionless scheduling, digital intake, and asynchronous messaging directly via web interfaces to permanently eliminate application installation barriers.
- Clinical Delivery Layer: Executing synchronous video visits, asynchronous electronic consults, remote monitoring, and virtual rounding. Systems must pull historical clinical context directly from the EHR and push finalized documentation back instantly.
- Clinical Intelligence Layer: Mandating algorithmic risk stratification, triage logic, and strict alert routing to ensure high acuity virtual encounters receive immediate clinical prioritization over basic queue processing.
- Enterprise Integration: Mandating FHIR-compliant APIs to fuse virtual platforms with existing pharmacy, billing, and imaging systems to drive absolute data fluidity without manual intervention.
- Revenue Cycle Operations: Automating charge capture, precise telehealth modifier logic, and aggressive claims scrubbing to ensure absolute billing compliance and instantly capture all virtual revenue.
- Analytics and Governance Layer: Demanding total operational visibility through utilization tracking, exact outcome measurement, quality metric capture, and automated audit logging. This transforms virtual care from a reactive departmental initiative into a strictly governed enterprise program.
This Is Where Virtual Care Starts to Fail
Without tight integration across these layers, workflows slow down and value drops. DASH ensures everything stays connected, fast, and reliable.
See How DASH Solves ItCore Components of Virtual Care Systems
Executing a scalable virtual care infrastructure requires specific operational capabilities. Gaps in any single component instantly create systemic bottlenecks. To prevent stalled deployments, executive leadership must mandate five core structural requirements:
- Vendor Agnostic Communication Architecture
Abstracting the video layer from the core clinical platform ensures communication technology upgrades occur without destroying established workflows. Fusing telehealth integration directly to a single vendor video SDK guarantees structural fragility within the fastest evolving technology layer. - Physiologic Data Ingestion
Continuous physiologic data from remote monitors and wearables must flow natively into the core system. The platform must aggressively ingest, normalize, and intelligently route these metrics directly to care teams. Failing to execute this integration leaves remote data clinically useless. - Asynchronous Clinical Execution
High-volume workflows, including dermatology reviews, behavioral health check-ins, and medication management, require strictly asynchronous channels. This capability aggressively reduces clinician scheduling burdens while enforcing absolute clinical quality across non-synchronous encounters. - Care Pathway Automation
Pre-visit questionnaires, post-visit follow-up protocols, and clinical escalation triggers demand strict algorithmic automation governed by specific patient condition logic. Forcing care coordinators to manually initiate these pathways guarantees operational failure at scale. - Algorithmic Compliance Enforcement
Interstate compact participation, state-level prescribing rules, and provider credentialing must be strictly enforced at the platform level. Relying on manual compliance checks and legacy spreadsheets ensures massive regulatory exposure and permanent operational breakdown at scale.
Role of Interoperability in Virtual Care
The connective tissue of this entire digital ecosystem is data liquidity. Without aggressive virtual care integration, the most advanced remote monitoring devices and high-definition video portals are practically useless. The data must flow naturally and securely into the patient’s permanent medical record.
Systemic interoperability failures occur strictly because executives treat integration as a secondary IT objective rather than a foundational architectural mandate. Designing a scalable virtual framework requires making interoperability the primary objective from inception. Enterprise platforms must natively execute HL7 and modern FHIR standards to enforce bidirectional communication across all core hospital systems.
Furthermore, overcoming deep EHR integration challenges transforms static clinical records into active operational triggers. When remote monitoring hardware detects dangerous physiologic anomalies, true interoperability ensures the alert bypasses isolated third-party applications entirely. The digital architecture must instantly drive that critical data through the EHR directly to the mobile device of the specific on-call physician, instantly triggering life-saving clinical execution.
Benefits for Providers and Patients
Deploying scalable virtual care infrastructure forces immediate, quantifiable value across all operational dimensions of digital care delivery.
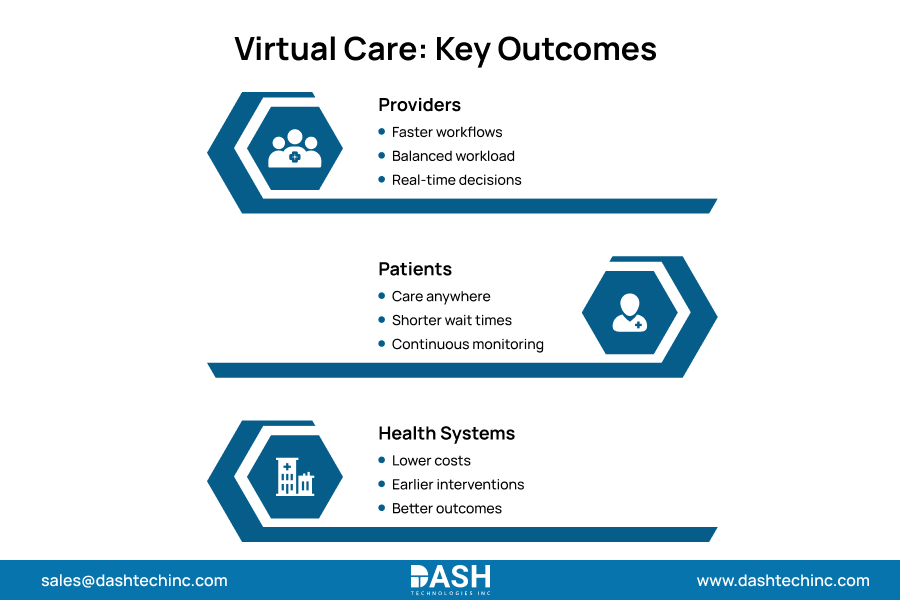
Provider Optimization
- Automated Efficiency: Accelerated operational throughput driven entirely by algorithmic workflows.
- Resource Maximization: Strict load balancing between virtual and physical encounters to protect physician bandwidth.
- Actionable Intelligence: Absolute data visibility empowering immediate clinical and operational decision making.
- Asymmetric Scaling: Exponentially expanding care models without requiring proportional staffing increases.
Patient Execution
- Unrestricted Access: Immediate clinical availability, completely independent of geographic location.
- Compressed Timelines: Drastically reduced wait periods for specialized medical consultations.
- Continuous Management: Unbroken care continuity enforced via persistent remote monitoring.
- Frictionless Engagement: Superior clinical adherence driven by intuitive digital communication tools.
Health System Dominance
- Cost Eradication: Aggressively reduced financial overhead across the total enterprise care delivery.
- Proactive Interventions: Superior clinical outcomes secured through rigorous predictive management.
- Value-Based Execution: Uncompromising structural support for advanced risk-bearing care models.
Conclusion
Telehealth deployment and virtual care infrastructure represent entirely different strategic realities. Launching a standalone video platform actively prevents the creation of a scalable digital care model. Facilities demand a rigid architectural foundation that enforces absolute integration, clinical continuity, and complete operational oversight across every care setting.
Executives must mandate virtual care as a core structural priority instead of a reactive IT tool. Hospitals investing in unified digital infrastructure permanently position themselves to expand enterprise reach, maximize operational efficiency, and guarantee connected clinical journeys.
Frequently Asked Questions
About Dash
Dash Technologies Inc.
We’re technology experts with a passion for bringing concepts to life. By leveraging a unique, consultative process and an agile development approach, we translate business challenges into technology solutions Get in touch.




