
How Hospitals Can Build a Scalable Healthcare Data Integration Layer?
Healthcare data integration is the infrastructure every hospital executive must get right before anything else scales. AI initiatives, analytics investments, and population health strategies all run on this foundation. Hospitals that have not addressed fragmentation are not simply behind technology. They are operating on a foundation that actively works against them.
Why Healthcare Data Fragmentation Is Still a Major Challenge?
Most hospital IT environments span dozens of separate clinical and administrative platforms. An emergency department system that cannot access the lab. A cardiology PACS is disconnected from the referring physician’s portal. A billing platform running on data two days old.
ONC’s Health IT Dashboard shows that most U.S. hospitals have adopted certified EHR technology. EHR adoption and hospital data integration are not the same problem. Systems that generate healthcare data silos continue producing isolated data, regardless of how many platforms a hospital has purchased.
Hospital interoperability challenges do not stem from bad intent. They stem from a decade of departmental procurement, system acquisitions, and legacy infrastructure layered on top of more legacy infrastructure. Each decision made sense in isolation. Collectively, they produced fragmented healthcare systems that resist standardization and make every downstream initiative harder to execute.
What Is a Healthcare Data Integration Layer?
A healthcare data integration layer is the interoperability of architecture tying to disparate clinical, administrative, and financial systems into a single coherent data environment. It goes beyond clinical data integration alone. It is not software you buy off a shelf. It’s a system designed to move, change, check, and send data throughout an organization instantly.
It sits between the EHR, imaging systems, revenue cycle platform, IoT devices, and analytics stack, translating between HL7 v2, FHIR R4, DICOM, and proprietary formats simultaneously. It enforces governance rules, ensuring the right data reaches the right system at the right moment, without manual intervention or the errors that manual intervention introduces.
Healthcare middleware includes engines, APIs, and transformation logic. It powers effective data pipelines. This technology helps hospitals automate data. In contrast, some hospitals still reconcile reports by hand each morning.
Common Sources of Data Fragmentation in Hospitals
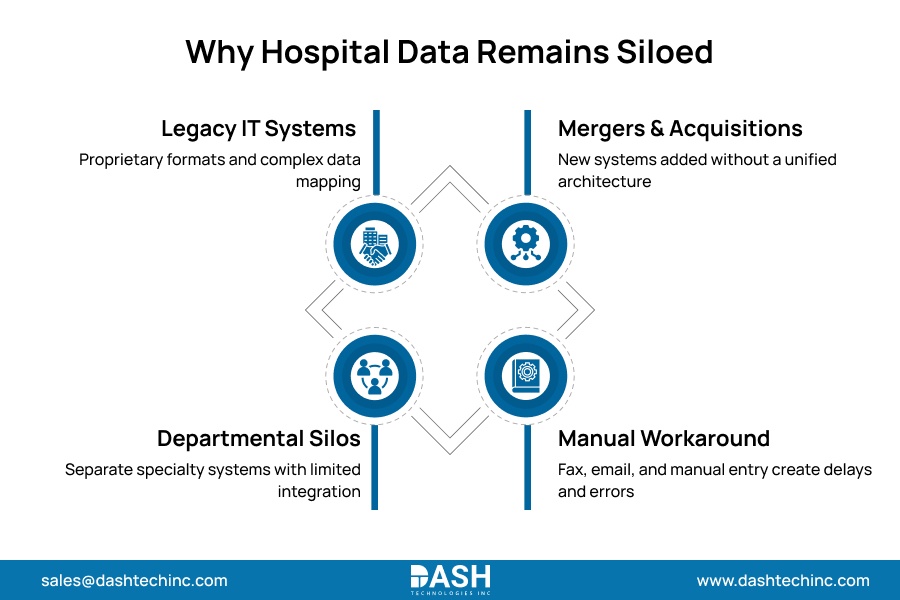
EHR integration challenges cause most hospital data issues, but they’re not the only problem. Several failure modes exist, and they compound each other.
Legacy IT environments predating modern interoperability protocols fundamentally reject cross-system communication by design. They generate data in proprietary formats. Modern enterprise platforms cannot consume this data without engineering highly complex purpose-built transformation layers.
Departmental procurement without enterprise architecture governance creates clinical data silos across each specialty. Cardiology, radiology, orthopedics, and the emergency department each select specialized platforms with no integration requirement built in. Each becomes a silo that every subsequent data request must work around.
Acquisitions and health system mergers add entire portfolios of disconnected healthcare systems overnight. Without an integration layer capable of absorbing them, complexity multiplies with every transaction.
When systems cannot communicate, staff compensate with fax, email, and manual data entry. Each workaround introduces error, latency, and compliance exposure that audits cannot fully recover. These failure modes do not exist independently. Each one amplifies the others.
Key Components of Healthcare Integration Architecture
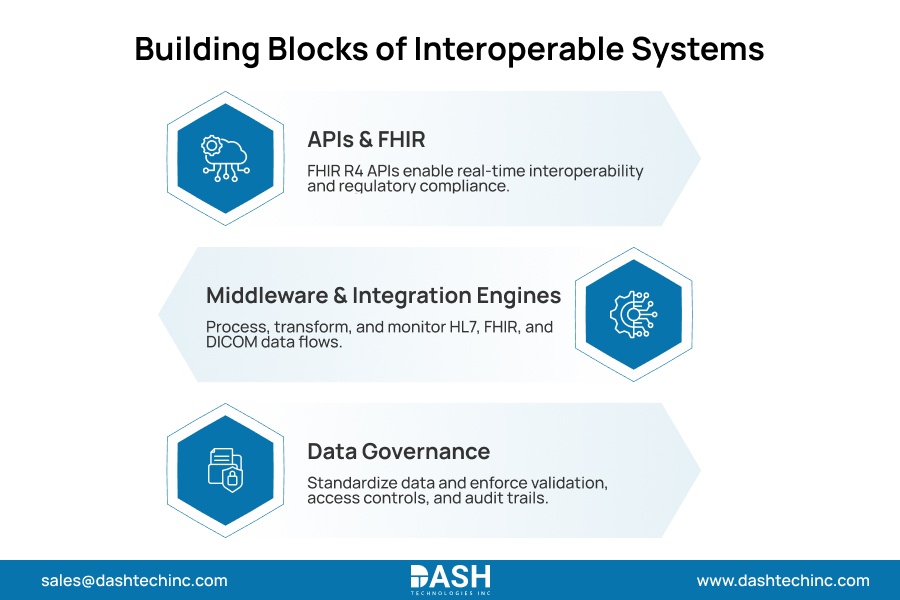
- APIs and FHIR-Based Integration:
FHIR R4 is now the primary standard for API integration in healthcare, and its adoption is not optional. CMS’s Interoperability and Patient Access Rule mandates FHIR-based APIs for payer-to-provider data exchange. Hospitals that resist FHIR adoption face regulatory exposure, not just technical debt.
FHIR enables real-time data exchange between clinical systems, patient-facing applications, and external platforms. Systems without native FHIR support require transformation logic to bridge the gap. That logic must be engineered deliberately, not assumed. - Middleware and Integration Engines:
Healthcare middleware is the operational core of any integration layer. It executes aggressive message routing, data transformation, strict queuing, automated error handling, and live alert generation across every clinical system.
Purpose-built healthcare integration platforms process the severe format complexity and transaction volumes that general enterprise tools completely fail to manage. They precisely parse HL7 v2 ADT feeds, structure DICOM headers, and distribute FHIR resources under extreme production loads. Organizations that build integration on general-purpose tools pay for it in outages, data loss, and engineering debt that grows over time. - Data Standardization and Governance:
Moving data represents merely half of the operational challenge. Guaranteeing absolute accuracy, consistent formatting, and strict auditability separates a functional integration layer from a massive compliance of liability.
A sound interoperability framework strictly dictates enterprise terminology standards like SNOMED CT, LOINC, and ICD-10 alongside data validation rules. It establishes unbreakable role-based access controls and permanent audit trails at every stage of the data pipeline. This is where healthcare data architecture does its real work. Governance built into the infrastructure enforces itself. Governance written into a policy document does not exist.
Modernize Your Healthcare Data Architecture
Build a robust healthcare integration foundation that improves interoperability, compliance, and operational efficiency
Schedule a ConsultationBenefits of a Unified Data Integration Layer
Executing this architecture delivers an immediate and concrete impact on healthcare operational efficiency. Clinical teams freed from manual reconciliation processes immediately shift those reclaimed hours toward direct patient care.
Operational workflows relying on delayed batch reports now trigger instantly upon live intelligence. Executive decision-making cycles that formerly required days now aggressively compress into mere hours.
Clinicians working from unified patient data make fewer preventable errors. Incomplete or stale data at the point of care contributes directly to adverse events that complete records prevent. That is not a marginal improvement. It is the most direct argument for integration investment that exists.
The picture sharpens executives, too. Revenue cycle anomalies surface as they happen. Service-line performance becomes visible through real-time healthcare analytics at a level of granularity that batch reporting never allowed.
And then there is regulatory exposure. CMS information blocking provisions under the 21st Century Cures Act carry real enforcement weight. Hospitals with a FHIR-compliant integration foundation turn that requirement into a structural advantage. Those managing fragmented systems face it as a growing liability.
How Hospitals Are Using Integration Layers to Enable AI and Analytics?
Healthcare AI infrastructure runs on data pipelines. Every predictive model and every clinical decision support tool require clean, normalized, high-volume data to function at scale. Population health platforms face the same ceiling. Without a working integration layer, none of these capabilities survives a pilot.
Health systems that have built integration architectures feeding enterprise data warehouses and healthcare analytics platforms in real time are already seeing the results. Sepsis prediction models pull ADT feeds, lab results, and vitals simultaneously. Readmission risk engines ingest discharge summaries alongside social determinants’ records. Population health platforms aggregate data from dozens of ambulatory sites into a single analytics layer.
The health systems achieving results from these platforms built the data infrastructure first. AI came second, not first. That sequence is not accidental.
Best Practices for Building Integration Strategy
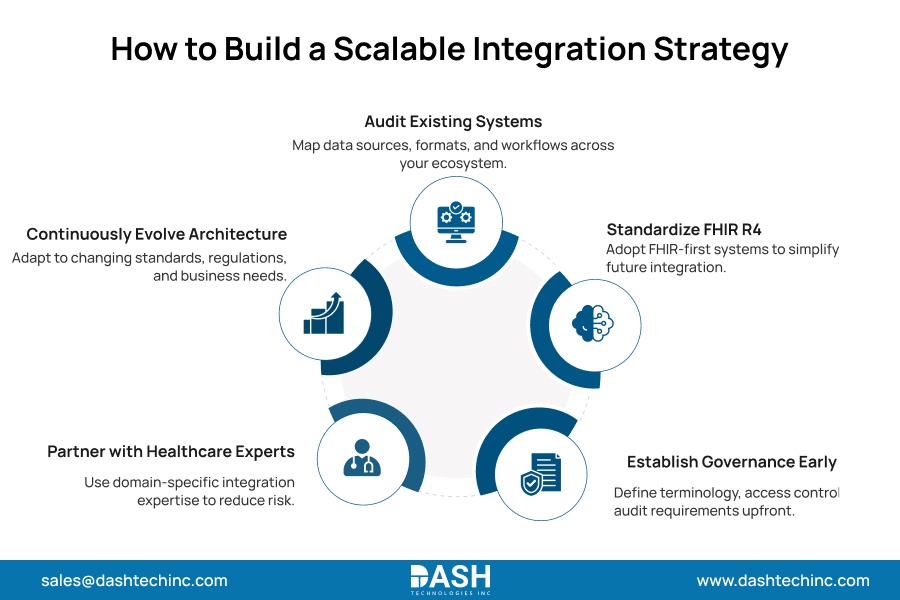
Hospitals conquering this integration bottleneck deploy uniform execution frameworks. These aren’t secrets. They show what makes a healthcare modernization strategy successful versus those that fail after launch.
Initiate an absolute audit of every system within the digital environment. Identify all generated data, proprietary data formats, and exact downstream consumption pathways. Invisible operational gaps actively prevent enterprise integration.
Mandate FHIR R4 compliance as a baseline requirement in every new system procurement. Scalable healthcare systems are built from compliant components at the outset, not retrofitted after. Retrofit projects are expensive and disruptive.
Setting governance before scale makes it hard to enforce. Terminology standards, access controls, and audit requirements applied retroactively to a large, active integration layer are difficult to get right consistently. The time to establish them is before the data volumes make them hard to reach.
Work with Dashtech’s interoperability engineering team rather than general IT vendors, adapting generic middleware to healthcare’s data complexity. The difference shows the production scale.
Execute permanent architectural evolution. Evolving HL7 versions, dynamic FHIR updates, aggressive regulatory mandates, and a volatile system that requires continuous structural adaptation. Facilities that inevitably fail completely halt their infrastructure investment directly after the initial operational launch.
Conclusion
Healthcare data integration determines whether a hospital’s clinical and operational systems work together or against each other. Fragmented systems do not just slow down analytics. They generate error, compliance exposure, and operational drag that compound over time.
The health systems leading their markets did not treat integration as the precursor to their AI and analytics investments. It was an investment.
If your organization is ready to address fragmentation at the infrastructure level, contact our engineering team to build the integration architecture your clinical and operational systems depend on.
Frequently Asked Questions
About Dash
Dash Technologies Inc.
We’re technology experts with a passion for bringing concepts to life. By leveraging a unique, consultative process and an agile development approach, we translate business challenges into technology solutions Get in touch.






