
Why Hospital Interoperability Projects Fail and How to Fix Them?
Even with billions spent on digital health in the past decade, hospital interoperability challenges still remain the top frustration for clinical and administrative leaders today. Most hospitals already have no shortage of technology, data, or software vendors. The real problem is that core systems still do not work together in a way that supports care, operations, and financial performance as one connected model.
That disconnect shows up everywhere. Clinical teams chase information across systems. Leaders rely on delayed reports pulled from multiple sources. Revenue teams try to reconcile activity that should already be visible. Even when hospitals invest heavily in digital platforms, healthcare data silos continue to block the outcomes those investments were supposed to deliver.
Interoperability is no longer just an IT objective. It is a strategic requirement for providers trying to improve care coordination, reduce operational friction, and make better use of enterprise data. Modern healthcare providers who treat interoperability as a side project often struggle. Hospitals that treat it as infrastructure are the ones that scale.
What Interoperability Means in Modern Hospitals?
Securing absolute healthcare interoperability demands far more than basic technical connectivity; it dictates the immediate, usable exchange of enterprise intelligence across all operational structures. It needs a unified data system. This system combines clinical, operational, and financial information. With it, hospitals can make real-time decisions for admin and medical care.
At a basic level, interoperability strictly mandates seamless EHR integration, continuous lab connectivity, live ADT feeds, and unified scheduling, billing, and departmental platforms. However, raw technical connectivity consistently fails to deliver ROI. System leadership must enforce strict data standardization and governance to prevent FHIR and HL7 integration issues from corrupting cross-functional data usability.
True structural interoperability helps facilities work better across departments. It improves care coordination. It also supports predictive risk models and automates clinical workflows.
A fully interoperable enterprise guarantees immediate, high-fidelity answers to four operational imperatives:
- What occurred clinically?
- What transpired operationally?
- What was the financial impact?
- What exact clinical action is required next?
When these insights remain trapped in isolated, fragmented systems, the facility’s operational capacity is fundamentally compromised.
Why Interoperability Projects Fail?
Addressing fundamental interoperability challenges healthcare executives face requires permanently abandoning fragmented technology strategies. Integration initiatives routinely fail due to structural operational deficits rather than technical limitations.
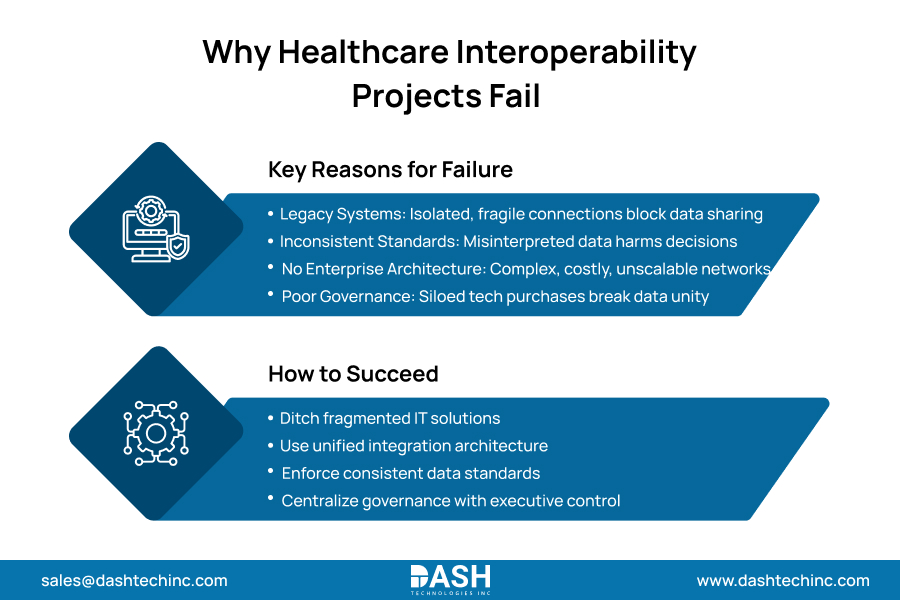
To secure absolute enterprise data fluidity, hospital leadership must entirely mitigate four primary failure modes:
- Legacy System Isolation: Decades of accumulating proprietary technology create environments fundamentally hostile to data exchange. Operating hundreds of isolated applications via fragile point-to-point connections guarantees integration failure whenever a single system updates. This isolation actively prevents comprehensive patient visibility.
- Inconsistent Data Standards: Nominal support for interoperability standards does not guarantee usability. Inconsistent implementations, non-standard extensions, and conflicting code sets mean data transfers arrive completely misinterpreted. This creates a dangerous illusion of connectivity while actively degrading clinical decision-making capabilities across the organization.
- Absence of Enterprise Architecture: Approaching integration as a series of isolated bilateral connections is a critical strategic error. Without a centralized integration layer, facilities inevitably build a complex, fragile web of connections. This infrastructure destroys budgets through exorbitant maintenance costs and strictly prohibits future scalability.
- Governance Deficits: Data ownership, standards of authority, and strict integration prioritization require centralized, uncompromising executive control. Allowing fragmented hospital departments to execute independent, siloed technology purchases actively destroys the unified enterprise data environment.
Overcoming these systemic barriers requires abandoning ad hoc, isolated IT solutions. Executives must mandate unified integration architecture, enforce strict semantic data standards, and absolutely centralize technology governance. This permanently eradicates operational silos and guarantees absolute long-term data exchange interoperability success.
The Real Impact of Poor Interoperability
Poor interoperability creates visible and invisible costs across the hospital. The visible costs are easier to spot delayed data access, duplicated work, reporting lag, and interface maintenance. The invisible costs are often more damaging because they affect how the organization functions every day.
One impact is delayed care. When clinicians cannot easily access complete patient information, they spend time searching, calling, documenting twice, or making decisions with partial context. This slows care pathways and increases reliance on manual coordination.
Another impact is revenue leakage. Charges might be delayed. Documentation may not match across systems. Also, utilization of data could take time to link with reimbursement logic. Even if clinical work is done well, weak integration can still reduce how efficiently the organization captures value from that work.
Workflow breakdown is another major issue. Departments often create manual fixes to compensate for missing interoperability. Workarounds help the system run. But they cause inconsistency. They add staffing burdens and increase operational risk. Over time, hospitals start managing the integration problem instead of solving it.
You can see this dynamic clearly in specialty workflows. In radiology, disconnected systems make data movement harder across the care continuum, which is why radiology interoperability has become such a strategic topic. In cardiology, workflow gaps across procedural and follow-up settings make coordination harder than it should be, as explored in From Cath Lab to Follow-Up: Closing Data Gaps in Cardiology Workflows. Orthopedic programs face similar issues when service-line data is spread across clinical, operational, and financial systems, as outlined in Breaking Down Data Silos in Orthopedic Departments.
How to Fix Interoperability at Scale?
Executing a successful EHR integration strategy demands abandoning fragmented interfaces for a centralized operational architecture. True scalability requires executives to ask “Which decisions, processes, and care transitions are breaking because data is not connected?” instead of “Which systems should connect?”. Establishing absolute data fluidity requires enforcing three rigorous architectural mandates:
Workflow Driven Integration: Aligning technical connectivity strictly with broken operational processes to guarantee immediate clinical outcomes.
Standardized API Architecture: Mandating FHIR protocols and API first frameworks to permanently eliminate brittle custom interfaces and ensure future scalability.
Absolute Data Standardization: Enforcing universal semantic definitions across all clinical events, locations, and procedures to prevent dangerous data misalignment.
Without strict enterprise data governance, connectivity remains fundamentally useless. Hospital leadership must enforce shared reference data and unified domain ownership to maintain absolute interoperability trust. This uncompromising approach permanently secures operational dominance.
Technology Stack Required for Modern Interoperability
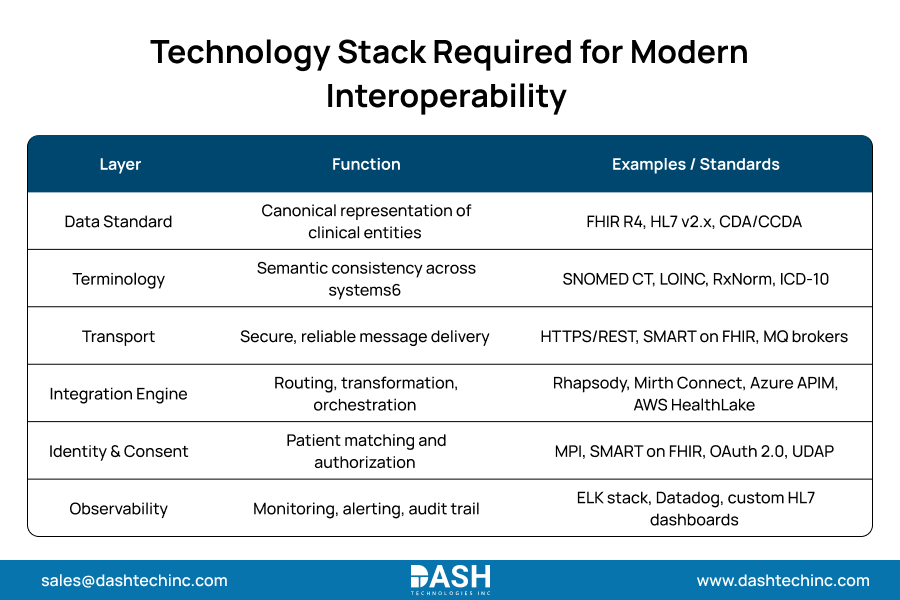
A modern interoperability strategy relies on a coordinated tech stack, not just one platform.
That stack often includes:
- Integration engines and interface management tools.
- API management layers for modern application connectivity.
- FHIR servers or interoperability layers.
- Master data and identity resolution capabilities.
- Data normalization and transformation services.
- Enterprise analytics environments.
- Monitoring and governance tools for interface health and data quality.
Healthcare integration platforms are most effective when they sit inside a clear architectural model. Without that model, hospitals just add technology to existing problems instead of fixing them.
This is where healthcare organizations often need both technical depth and strategic guidance. The challenge is not simply choosing products. It is designing how those products support the larger hospital data integration strategy over time.
Conclusion
Interoperability is not a side of initiative. It is a system-wide transformation layer that determines whether hospital technology investments actually work together. When interoperability projects fail, the cause is usually not technology alone. It is a lack of architecture, standards of discipline, enterprise ownership, and strategy aligned to operational reality.
Hospitals that succeed take a different approach. They build interoperability as an infrastructure. They standardize data before scaling use cases. Hospitals connect systems in ways that support care, workflows, analytics, and financial performance together.
That is also why the right partner matters. Hospitals do not just need interface delivery. They need an integration partner and an architecture expert who can help design scalable interoperability across the enterprise. Contact us to partner with us!
Frequently Asked Questions
About Dash
Dash Technologies Inc.
We’re technology experts with a passion for bringing concepts to life. By leveraging a unique, consultative process and an agile development approach, we translate business challenges into technology solutions Get in touch.





