Hospital IT Modernization: A Practical Roadmap for Legacy System Transformation
Hospital IT modernization determines what a health system can be operationalized. Not over a five-year horizon, right now. The infrastructure decisions made today govern which AI tools deploy, which analytics programs run, and which care coordination workflows execute at clinical volume.
Health systems operating on legacy architecture are not just behind technology. They are behind every clinical initiative that requires data infrastructure to function. Most CIOs understand this. The ones who acted on it three years ago are not managing the same pressure.
Why Legacy Systems are Slowing Healthcare Innovation?
Healthcare legacy systems were designed for different operating models. Clinical documentation, billing, scheduling, and imaging: each solved one workflow at one point in time. Real-time data exchange across the rest of the hospital stack was never part of the design. The architecture reflects exactly that.
Outdated hospital infrastructure creates friction everywhere it touches. Clinicians waiting on batch-processed lab results. Care teams working from incomplete records because the scheduling system and the EHR do not talk. Revenue cycle staff reconciling figures by hand, which the two systems should reconcile automatically. Not a technology curiosity. Operational drag, compounding with every quarter, the legacy stack stays in place.
Unlock Real-Time Healthcare Data
Connect legacy platforms and eliminate data silos to improve care coordination, operational efficiency, and decision-making across your organization.
Talk to Our ExpertWhat Hospital IT Modernization Really Means?
Hospital systems cannot replace core EHR infrastructure on an operationally survivable timeline. Any viable healthcare modernization strategy must be built directly from that strict constraint. The practical path requires retiring obsolete systems and API-wrapping salvageable applications to engineer a connective architecture. This forces the disjointed environment to function as a unified interoperable platform.
A 2021 ONC Report to Congress noted non-federal acute care hospital EHR adoption hit 96%. The report identified interoperability gaps as the primary barrier preventing organizations from extracting clinical and operational value from those massive investments. System integration remains the true operational bottleneck.
Digital transformation in healthcare means treating the stack as infrastructure. Not as a project with a delivery date and a post-go-live handoff. The requirements change. The regulatory environment changes. A modernization program that does not plan for continuous evolution delivers a legacy system with a newer timestamp.
Common Challenges in Modernizing Hospital Systems
Modernizing hospital infrastructure forces engineering teams to confront strict operational constraints. The core healthcare IT challenges follow predictable patterns across nearly every facility. Data migration consistently operates as the most expensive phase.
Transporting clinical histories and claims data from legacy formats into modern environments without triggering data loss or integrity failures demands exact execution. This specific phase forces the majority of schedules and budget overruns.
System migration healthcare projects must directly account for two additional baseline risks:
Security exposure: Modernization surfaces the severe vulnerabilities hidden within decaying infrastructure. The HHS Office for Civil Rights tracks breach volumes directly correlating to legacy platforms running end-of-life software during active transition windows. Security engineering must run simultaneously with migration. Delaying this step actively builds the exact vulnerabilities the project intends to destroy.
Operational disruption: Clinical teams conditioned by legacy interfaces reject sudden workflow shifts. Engineering go-live cutovers require strict alignment with live patient census data. Poorly executed transitions at high-volume facilities immediately paralyze care delivery.
These represent standard execution risks. Any viable architectural strategy factors in these absolute constraints long before deployment begins.
Key Technologies Driving Healthcare IT Modernization
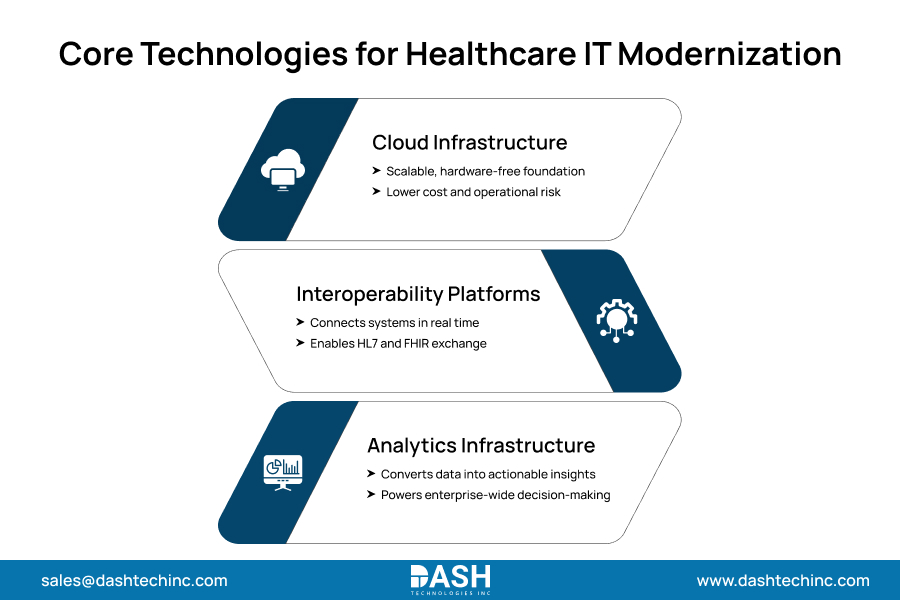
Cloud-native healthcare systems establish the core architectural foundation. Deploying to the cloud removes physical hardware maintenance and manual capacity planning as active IT burdens. Managed, scalable infrastructure that adapts to clinical demand without a procurement cycle. Hospitals still running physical data centers bear operational costs and failure risks that cloud infrastructure eliminates.
Interoperability platforms handle what the cloud cannot. FHIR-based APIs, integration engines, and middleware layers ensure that systems now running in the cloud environment exchange data correctly, in real time, across clinical and administrative workflows. Without this layer, cloud migration moves the legacy stack to a different location. The integration problem stays exactly where it was.
Healthcare analytics infrastructure guarantees the final operational output. Live data pipelines and massive clinical data warehouses strictly require an interoperable foundation to execute at scale. Facilities upgrading their architecture without natively instrumenting the analytics layer to build entirely dormant capabilities. This structural oversight immediately forces massive architectural failure across the enterprise.
Step-by-Step Roadmap for Legacy System Transformation
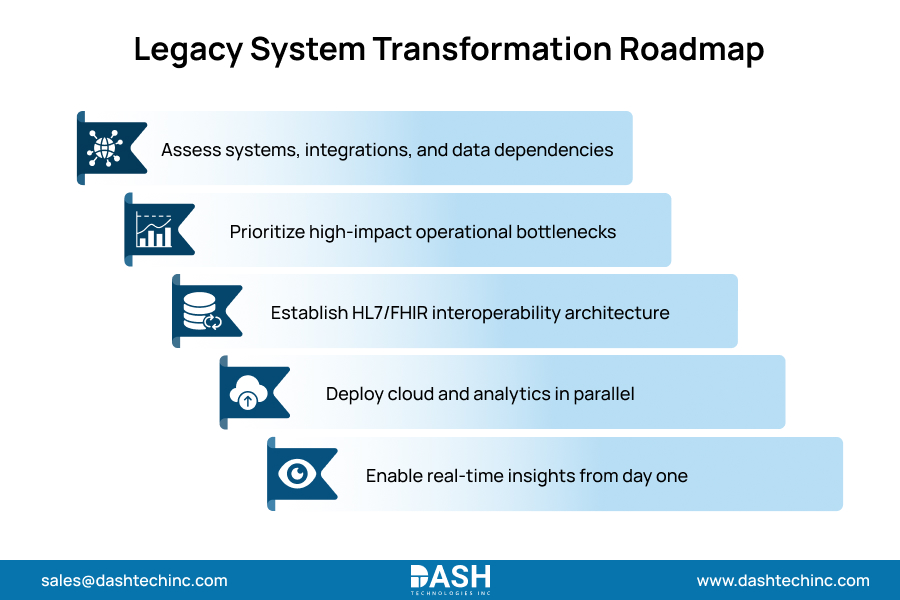
Healthcare modernization of roadmap execution follows a consistent structure across health systems that completes it without derailing operations. Sequencing is not arbitrary. Each phase creates the preconditions that the next one requires.
- Assess Existing Infrastructure
Start with a complete technical inventory. Every system is in production. Every integration point. Every data dependency. Organizations that skip this step regularly discover mid-migration that a system marked for retirement feeds three others they never mapped. The assessment is not optional. It is the decision foundation for everything else rests on, and it almost always surfaces technical debt that IT leadership had not communicated to the board. - Prioritize High-Impact Systems
Not everything modernizes at the same time. High-impact systems are where legacy constraints create the most measurable friction right now. Revenue cycle. Care coordination. Clinical documentation. Lab data flows.
These are the areas where the hospital’s digital transformation strategy delivers the fastest results. Sequence from highest friction to lowest. Projects that go in the other direction lose executive support before they reach the systems that actually matter. - Enable Interoperability
Define the interoperability architecture before any system migration begins. FHIR API standards. Integration of engine selection. Data governance requirements. These need resolution before system-specific migration starts, not after. A modern system migrated without an interoperability framework is as isolated as the legacy system it replaced. Different infrastructure, same problem. - Implement Cloud and Analytics Layers
Cloud migration and analytics infrastructure are built together. Not sequential. The analytics layer must be instrumented from the start of cloud deployment. Organizations that plan to add analytics after stabilization find that the stabilization phase has no defined end. By the time the environment is stable enough, the data architecture is locked into patterns that require significant rework to instrument correctly.
How Hospital IT Modernization Improves Clinical and Operational Performance?
The gains show up fast once the stack works. Clinicians stop waiting. Documentation runs where the care happens. Orders do not get lost in handoffs between systems that have no idea the other exists. Staff hours that used to go into manual reconciliation go somewhere else. The hours recovered per clinical FTE compound over quarters, not years.
Real-time data access changes care delivery in ways batch-processed systems cannot replicate. Integrated clinical decision support catches risks that fragmented records miss. The difference is not marginal.
Population health programs, AI-assisted care tools, predictive analytics: one prerequisite. An infrastructure layer that functions. Health systems running high-volume acute care and specialty networks see this most clearly because those environments generate data volume where integration failures do the most damage.
Modern infrastructure is not a downstream benefit. It is what care delivery actually runs on.
Conclusion
Organizations that frame hospital modernization as an IT project get IT-project results. Not fundamentally different operational capacity. The ones that frame it as a capital infrastructure decision, same category as a new facility or a major equipment acquisition, plan and fund it at the right scope. That difference is visible in outcomes.
Simply put, every year a legacy system runs; it costs more to maintain. It also becomes tougher to update and protect. Scalable architecture and real interoperability are not aspirational targets. They are the baseline requirement for any health system operating at volume.
If your organization is planning or executing a modernization program, Dashtech’s healthcare IT strategy team works with hospital leadership from initial infrastructure assessment through full implementation, ensuring the architecture holds up under the operational demands it will face.
Frequently Asked Questions
About Dash
Dash Technologies Inc.
We’re technology experts with a passion for bringing concepts to life. By leveraging a unique, consultative process and an agile development approach, we translate business challenges into technology solutions Get in touch.