Building SaMD (Software as a Medical Device): Architecture, Compliance, and Challenges
Software as a Medical Device draws a hard regulatory line. Most engineering teams miss it until it costs them. Standalone clinical software performing a medical function (diagnostic decision support, treatment recommendation algorithms, patient monitoring tools) falls under FDA and MDR jurisdiction. Hardware involvement does not change that. That mandates a completely different development process. Validated architecture, documented risk management, & Cybersecurity controls are built in from day one. Treat SaMD development like standard software development, and you find the gap during FDA review, & the regulatory clock does not pause for architectural rework.
What is Software as a Medical Device (SaMD)?
SaMD meaning: medical device software executing specific medical purposes entirely independent of hardware. The IMDRF defined this category, and the FDA codified the framework directly within its Software as a Medical Device guidance. Whether deploying clinical decision support engines for diagnostic conclusions or utilizing patient monitoring medical device software to trigger care escalation, these systems fall squarely under this classification. All of it is subject to premarket review, post-market surveillance, and quality system regulation. The software-only classification does not reduce regulatory burden. It specifies it.
Why SaMD Adoption is Growing Rapidly?
Digital therapeutics, AI medical software, and connected healthcare devices created an entire category of regulated software that operates outside physical device boundaries. FDA has cleared a growing roster of AI/ML-enabled medical devices through 510(k) and De Novo pathways. Remote monitoring. Clinical AI in EHR workflows. Prescription digital therapeutics are replacing or augmenting pharmacological treatment. Payers followed outcomes of data into reimbursement coverage. Physicians accepted software-driven clinical inputs when evidence was held. The market grew because compliant SaMD delivered clinical results. Not because the compliance was easy.
Core Architecture Components of SaMD Platforms
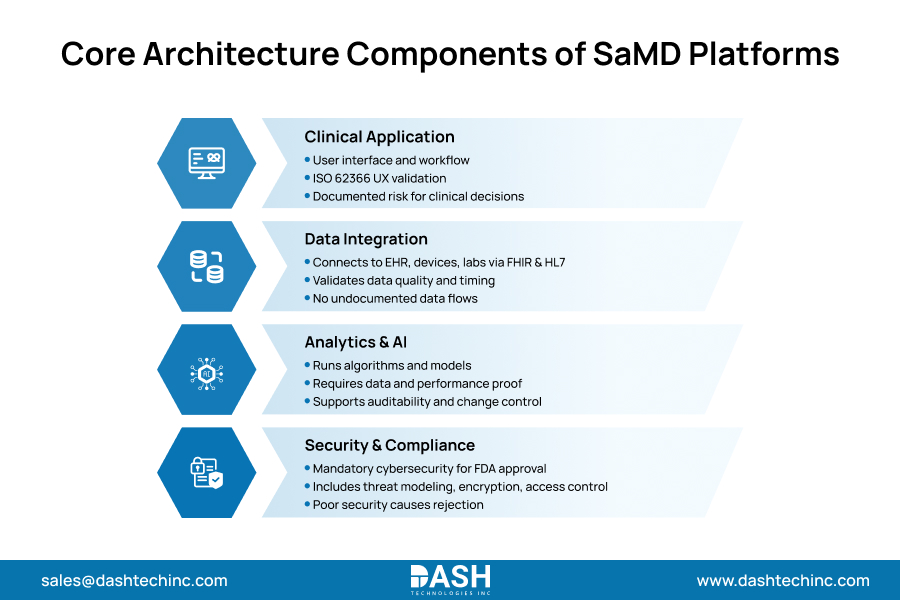
Four structural layers govern every SaMD architecture. Healthcare cloud architecture sits under all of it. Clinical application, data integration, analytics, and AI, security. Modern medical software platforms build on that structure. Each layer performs independently and connects.
- Clinical Application Layer
Interface and workflow logic for clinical inputs and decision outputs. Manages user interaction across device types and care settings. UX validation requirements under ISO 62366. Every interaction that influences a clinical decision is a documented risk item. Not a design preference. A regulatory artifact. Usability validation testing must produce objective evidence before submission. - Data Integration Layer
Connects the SaMD platform to EHRs, connected devices, labs, and imaging systems via FHIR APIs and HL7 standards. Every data source introduces integration risk that the validation process must account for. Data provenance, format consistency, and latency tolerances all require explicit specification. Undocumented data flows are audit liabilities. The integration architecture is a regulatory boundary condition, not a technical convenience. - Analytics and AI Layer
Where diagnostic algorithms, predictive models, and clinical scoring engines run. FDA treats AI/ML-enabled SaMD as a distinct regulatory pathway requiring algorithm training data documentation, performance benchmarks, and output confidence thresholds. Continuous learning models introduce additional change control obligations under FDA’s predetermined change control plan framework. Build this layer with auditability as a core requirement. Algorithm performance that cannot be audited cannot be defended in a submission. - Security and Compliance Layer
Cybersecurity controls are premarket submission requirements. No optional features. FDA medical device cybersecurity guidance mandates threat modeling, software bill of materials, and vulnerability management processes before submission. Encryption, access controls, audit logging, and incident response protocols are evaluated during review. A SaMD platform with an inadequate security architecture does not receive conditional clearance. It gets rejected. The rebuild cost is not a security investment. It is a preventable failure.
Build Audit-Ready SaMD Integrations
Design compliant, scalable integration layers across EHRs, labs, imaging systems, and connected devices.
Connect With ExpertsRegulatory and Compliance Requirements for SaMD
FDA medical software compliance starts with risk classification. Low-risk SaMD: 510(k) or exempt. Higher risk: De Novo or PMA, with clinical validation data required. MDR compliance healthcare: CE marking under Regulation 2017/745. Post-market clinical follow-up standards that exceed legacy MDD. Two frameworks. Different submission mechanics. Same foundational requirement: quality system, validation-ready architecture, before touching submission paperwork.
ISO 13485 and IEC 62304 documentation are mandatory under both regimes. SaMD validation starts with architecture. Design controls, ISO 14971 risk management, traceability matrices linking every requirement to test evidence: these are architecture-level decisions. No paperwork was added at the end. Teams that plan validation late find that their architecture does not support it. That is a rebuild and not a fix.
Common Challenges in Building SaMD Solutions
Healthcare software challenges show up fast. SaMD-regulated software development does not work like standard engineering. Clinical scales make the gap visible. Most teams find this out mid-project.
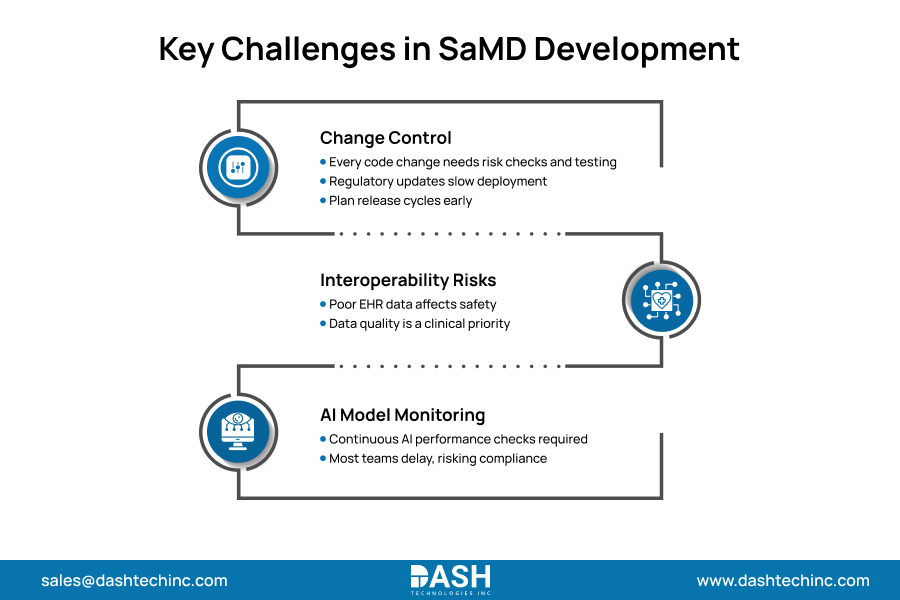
Change control is the first barrier. Every code of change in a regulated environment requires documented risk assessment, regression testing, and, in many cases, regulatory notification. CI/CD pipelines that work in consumer software run into validation cycle constraints in a medical device context. Deployment cadence planning must account for this from sprint one.
Interoperability introduces patient safety exposure. SaMD clinical algorithms producing outputs from incomplete or malformed EHR data are not software bugs. They are adverse event risks. Data quality governance is a patient safety function, not an IT task.
AI model performance degradation in deployed SaMD creates post-market surveillance obligations most development teams have not instrumented for. FDA expects continuous monitoring. Most SaMD architectures do not build that in from day one. They plan to add it later. Later never arrives on schedule.
Best Practices for Scalable and Compliant SaMD Development
Start with design controls or restart the project later. That is the actual choice. V-model and agile-with-gates processes both require design inputs, design outputs, and V&V documentation at every stage. Skip it, and the review process sends you back. Not a delay. A restart.
Scalable medical software. Validation-ready architecture is a design constraint, not a feature. Modular components. Explicit interfaces. Full traceability from requirements to test cases. Configuration management that an auditor can follow. Every dependency documented. Every third-party library is assessed before it enters the codebase. These decisions happen in sprint planning, not the remediation phase.
Security runs concurrently. Secure healthcare software development means threat modeling, SBOM, and penetration testing as premarket submission deliverables. Schedule them as engineering work, not QA cleanup. They belong in the sprint, not the backlog.
The SaMD programs that clear on first submission are the ones where regulatory and engineering share the same sprint plan. Separate tracks produce rework. That separation is where most programs lose their schedule.
Conclusion
Get the architecture right from the start or rebuild it under regulatory pressure. Two paths. Organizations that retrofit compliance onto completed SaMD systems pay twice. Once for the build. Once for the rework. The ones that build right clear first submission and ship, while others are still in remediation. That investment belongs before the first sprint, not after the first FDA rejection.
Dashtech’s MedTech engineering team works with organizations designing and building regulated medical software, from architecture review through FDA submission support. Build it right the first time.
Frequently Asked Questions
About Dash
Dash Technologies Inc.
We’re technology experts with a passion for bringing concepts to life. By leveraging a unique, consultative process and an agile development approach, we translate business challenges into technology solutions Get in touch.